

Direct hospital costs of chest pain patients attending the emergency department: a retrospective study
- PMID: 16674827
- PMCID: PMC1488872
- DOI: 10.1186/1471-227X-6-6
Direct hospital costs of chest pain patients attending the emergency department: a retrospective study
Abstract
Background: Chest pain is one of the most common complaints in the Emergency Department (ED), but the cost of ED chest pain patients is unclear. The aim of this study was to describe the direct hospital costs for unselected chest pain patients attending the emergency department (ED).
Methods: 1,000 consecutive ED visits of patients with chest pain were retrospectively included. Costs directly following the ED visit were retrieved from the hospital economy system.
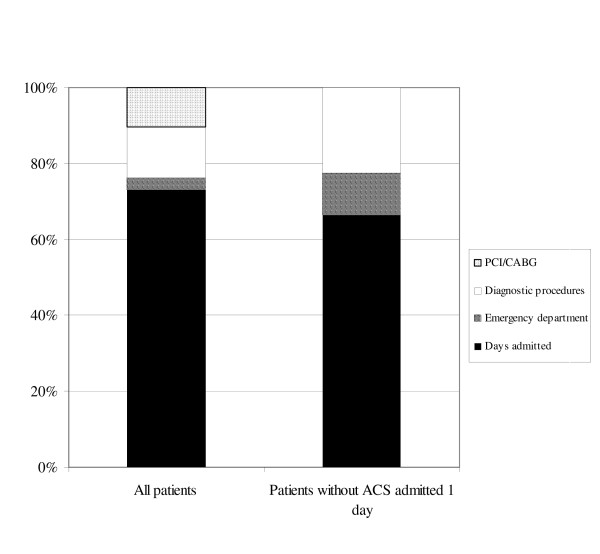
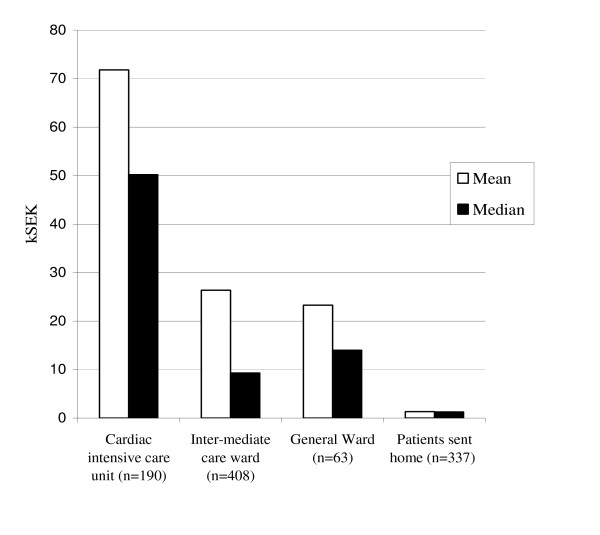
Results: The mean cost per patient visit was 26.8 thousand Swedish kronar (kSEK) (median 7.2 kSEK), with admission time accounting for 73% of all costs. Mean cost for patients discharged from the ED was 1.4 kSEK (median 1.3 kSEK), and for patients without ACS admitted 1 day or less 7.6 kSEK (median 6.9 kSEK). The practice in the present study to admit 67% of the patients, of whom only 31% proved to have ACS, was estimated to give a cost per additional life-year saved by hospital admission, compared to theoretical strategy of discharging all patients home, of about 350 kSEK (39 kEUR or 42 kUSD).
Conclusion: Costs for chest pain patients are large and primarily due to admission time. The present admission practice seems to be cost-effective, but the substantial overadmission indicates that better ED diagnostics and triage could decrease costs considerably.
Figures
References
-
- Tosteson AN, Goldman L, Udvarhelyi IS, Lee TH. Cost-effectiveness of a coronary care unit versus an intermediate care unit for emergency department patients with chest pain. Circulation. 1996;94:143–50. - PubMed
-
- Goodacre S, Nicholl J, Dixon S, Cross E, Angelini K, Arnold J, Revill S, Locker T, Capewell SJ, Quinney D, et al. Randomised controlled trial and economic evaluation of a chest pain observation unit compared with routine care. Bmj. 2004;328:254. doi: 10.1136/bmj.37956.664236.EE. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
