

Prognostic factors in solitary plasmacytoma of the bone: a multicenter Rare Cancer Network study
- PMID: 16677383
- PMCID: PMC1479355
- DOI: 10.1186/1471-2407-6-118
Prognostic factors in solitary plasmacytoma of the bone: a multicenter Rare Cancer Network study
Abstract
Background: Solitary plasmacytoma (SP) of the bone is a rare plasma-cell neoplasm. There are no conclusive data in the literature on the optimal radiation therapy (RT) dose in SP. Therefore, in this large retrospective study, we wanted to assess the outcome, prognostic factors, and the optimal RT dose in patients with SP.
Methods: Data from 206 patients with bone SP without evidence of multiple myeloma (MM) were collected. Histopathological diagnosis was obtained for all patients. The majority (n = 169) of the patients received RT alone; 32 chemotherapy and RT, and 5 surgery. Median follow-up was 54 months (7-245).
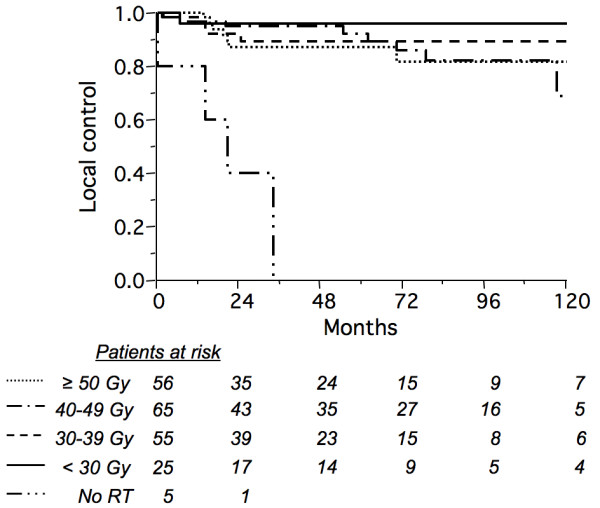
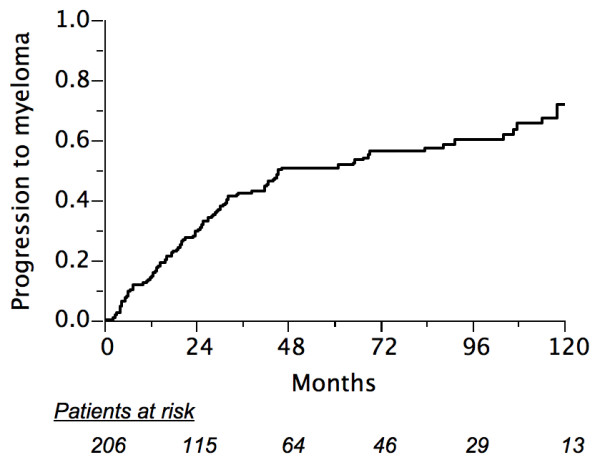
Results: Five-year overall survival, disease-free survival (DFS), and local control was 70%, 46%, and 88%; respectively. Median time to MM development was 21 months (2-135) with a 5-year probability of 51%. In multivariate analyses, favorable factors were younger age and tumor size < 5 cm for survival; younger age for DFS; anatomic localization (vertebra vs. other) for local control. Older age was the only predictor for MM. There was no dose-response relationship for doses 30 Gy or higher, even for larger tumors.
Conclusion: Younger patients, especially those with vertebral localization have the best outcome when treated with moderate-dose RT. Progression to MM remains the main problem. Further investigation should focus on adjuvant chemotherapy and/or novel therapeutic agents.
Figures
References
-
- Knowling MA, Harwood AR, Bergsagel DE. Comparison of extramedullary plasmacytomas with solitary and multiple plasma cell tumors of bone. J Clin Oncol. 1983;1:255–262. - PubMed
-
- Galieni P, Cavo M, Avvisati G, Pulsoni A, Falbo R, Bonelli MA, Russo D, Petrucci MT, Bucalossi A, Tura S. Solitary plasmacytoma of bone and extramedullary plasmacytoma: two different entities? Ann Oncol. 1995;6:687–691. - PubMed
-
- Jyothirmayi R, Gangadharan VP, Nair MK, Rajan B. Radiotherapy in the treatment of solitary plasmacytoma. Br J Radiol. 1997;70:511–516. - PubMed
-
- Brinch L, Hannisdal E, Abrahamsen AF, Kvaloy S, Langholm R. Extramedullary plasmacytomas and solitary plasma cell tumours of bone. Eur J Haematol. 1990;44:131–134. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
