

Endoscopic indications for endoscopic mucosal resection of laterally spreading tumours in the colorectum
- PMID: 16682427
- PMCID: PMC1860093
- DOI: 10.1136/gut.2005.087452
Endoscopic indications for endoscopic mucosal resection of laterally spreading tumours in the colorectum
Abstract
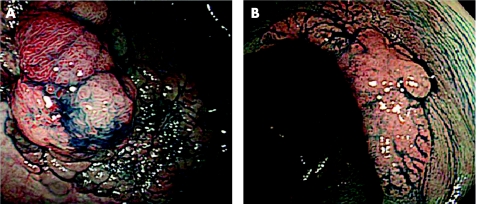
Background: Laterally spreading tumours (LSTs) in the colorectum are usually removed by endoscopic mucosal resection (EMR) even when large in size. LSTs with deeper submucosal (sm) invasion, however, should not be treated by EMR because of the higher risk of lymph node metastasis.
Aims: To determine which endoscopic criteria, including high magnification pit pattern analysis, are associated with sm invasion in LSTs and clarify indications for EMR.
Methods: Eight endoscopic criteria from 511 colorectal LSTs (granular type (LST-G type); non-granular type (LST-NG type)) were evaluated retrospectively for association with sm invasion, and compared with histopathological findings.
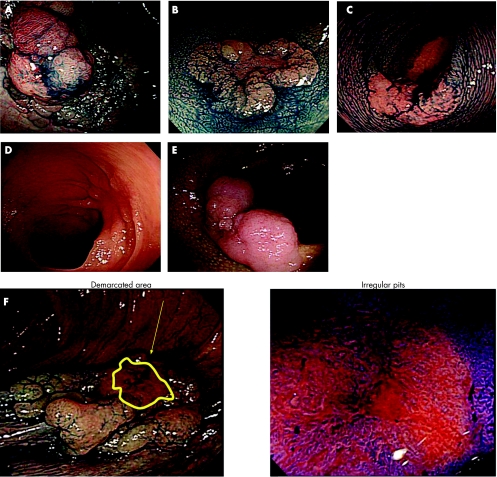
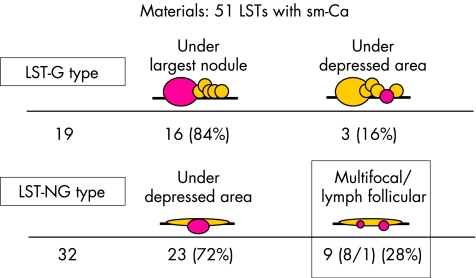
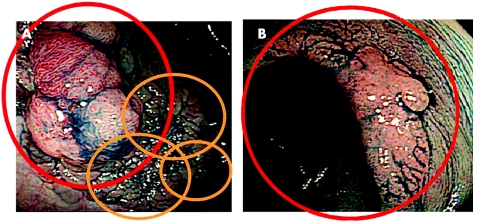
Results: LST-NG type had a significantly higher frequency of sm invasion than LST-G type (14% v 7%; p<0.01). Presence of a large nodule in LST-G type was associated with higher sm invasion while pit pattern (invasive pattern), sclerous wall change, and larger tumour size were significantly associated with higher sm invasion in LST-NG type. In 19 LST-G type with sm invasion, sm penetration determined histopathologically occurred under the largest nodules (84%; 16/19) and depressed areas (16%; 3/19). Deepest sm penetration in 32 LST-NG type was either under depressed areas (72%; 23/32) or lymph follicular or multifocal sm invasion (28%; 1/32 and 8/32, respectively).
Conclusions: When considering the most suitable therapeutic strategy for LST-G type, we recommend endoscopic piecemeal resection with the area including the large nodule resected first. In contrast, LST-NG type should be removed en bloc because of the higher potential for malignancy and greater difficulty in diagnosing sm depth and extent of invasion compared with LST-G type.
Conflict of interest statement
Conflict of interest: None declared.
References
-
- Kudo S. Endoscopic mucosal resection of flat and depressed types of early colorectal cancer. Endoscopy 199325455–461. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials