

Current management of the complications of portal hypertension: variceal bleeding and ascites
- PMID: 16682712
- PMCID: PMC1455434
- DOI: 10.1503/cmaj.051700
Current management of the complications of portal hypertension: variceal bleeding and ascites
Abstract
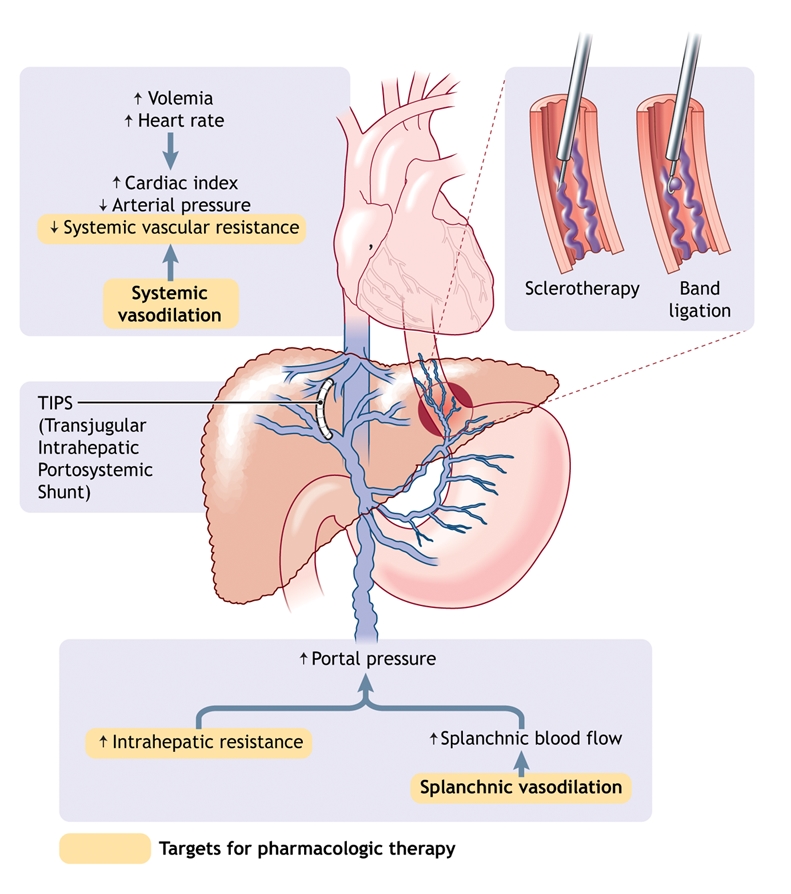
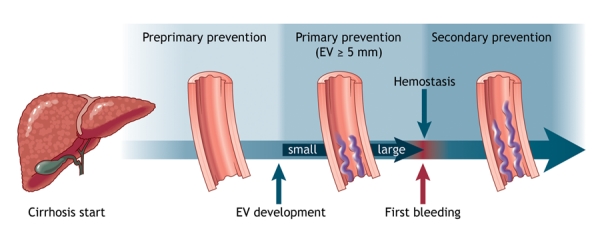
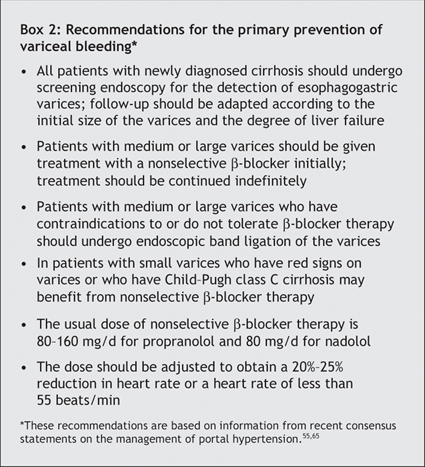
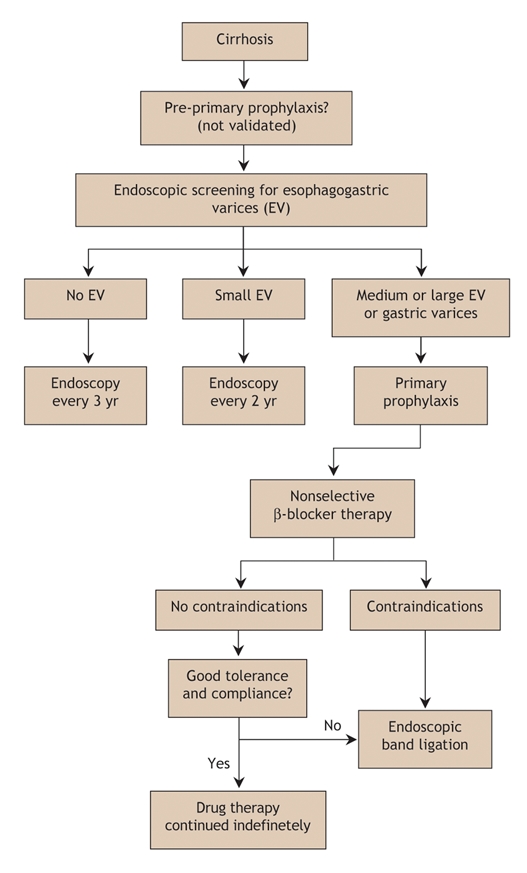
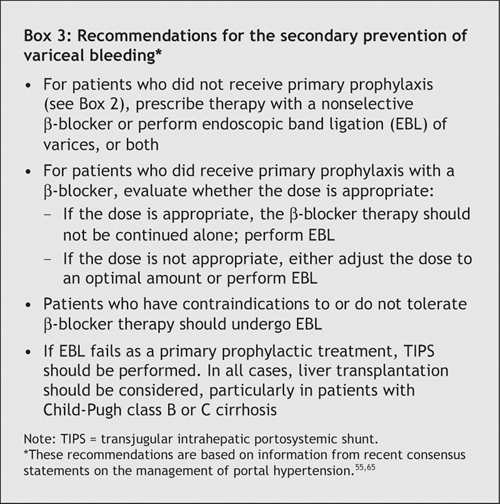
Portal hypertension is one of the main consequences of cirrhosis. It results from a combination of increased intrahepatic vascular resistance and increased blood flow through the portal venous system. The condition leads to the formation of portosystemic collateral veins. Esophagogastric varices have the greatest clinical impact, with a risk of bleeding as high as 30% within 2 years of medium or large varices developing. Ascites, another important complication of advanced cirrhosis and severe portal hypertension, is sometimes refractory to treatment and is complicated by spontaneous bacterial peritonitis and hepatorenal syndrome. We describe the pathophysiology of portal hypertension and the current management of its complications, with emphasis on the prophylaxis and treatment of variceal bleeding and ascites.
Figures
Similar articles
-
Management of ascites and hepatorenal syndrome.Hepatol Int. 2018 Feb;12(Suppl 1):122-134. doi: 10.1007/s12072-017-9815-0. Epub 2017 Aug 23. Hepatol Int. 2018. PMID: 28836115 Review.
-
Management of acute variceal bleeding.Dig Dis. 2003;21(1):6-15. doi: 10.1159/000071333. Dig Dis. 2003. PMID: 12837994 Review.
-
Pharmacologic therapy for gastrointestinal bleeding due to portal hypertension and esophageal varices.Curr Gastroenterol Rep. 2006 Feb;8(1):7-13. doi: 10.1007/s11894-006-0058-9. Curr Gastroenterol Rep. 2006. PMID: 16510029 Review.
-
Management of acute variceal haemorrhage.Eur J Gastroenterol Hepatol. 2001 Apr;13(4):335-42. doi: 10.1097/00042737-200104000-00006. Eur J Gastroenterol Hepatol. 2001. PMID: 11338059 Review.
-
Nonendoscopic management strategies for acute esophagogastric variceal bleeding.Gastroenterol Clin North Am. 2014 Dec;43(4):819-33. doi: 10.1016/j.gtc.2014.08.011. Epub 2014 Sep 27. Gastroenterol Clin North Am. 2014. PMID: 25440928 Free PMC article. Review.
Cited by
-
Outcomes of transjugular intrahepatic portosystemic shunts for ascites.Semin Intervent Radiol. 2014 Sep;31(3):248-51. doi: 10.1055/s-0034-1382792. Semin Intervent Radiol. 2014. PMID: 25177085 Free PMC article. Review.
-
Clinical application of partial splenic embolization.ScientificWorldJournal. 2014;2014:961345. doi: 10.1155/2014/961345. Epub 2014 Nov 3. ScientificWorldJournal. 2014. PMID: 25538966 Free PMC article. Review.
-
Effect of propranolol on the splanchnic and peripheral renin angiotensin system in cirrhotic patients.World J Gastroenterol. 2008 Nov 28;14(44):6824-30. doi: 10.3748/wjg.14.6824. World J Gastroenterol. 2008. PMID: 19058308 Free PMC article.
-
PPIs are not associated with a lower incidence of portal-hypertension-related bleeding in cirrhosis.World J Gastroenterol. 2010 Dec 14;16(46):5869-73. doi: 10.3748/wjg.v16.i46.5869. World J Gastroenterol. 2010. PMID: 21155009 Free PMC article.
-
Clinical Characteristics and Outcomes Associated With Distinct Hemodynamic Patterns in End-stage Liver Disease: A Retrospective Cohort Analysis.J Clin Exp Hepatol. 2024 Nov-Dec;14(6):101470. doi: 10.1016/j.jceh.2024.101470. Epub 2024 Jun 20. J Clin Exp Hepatol. 2024. PMID: 39100890
References
-
- Shibayama Y, Nakata K. Localization of increased hepatic vascular resistance in liver cirrhosis. Hepatology 1985;5:643-8. - PubMed
-
- Pinzani M, Gentilini P. Biology of hepatic stellate cells and their possible relevance in the pathogenesis of portal hypertension in cirrhosis. Semin Liver Dis 1999;19:397-410. - PubMed
-
- Rockey DC, Weisiger RA. Endothelin induced contractility of stellate cells from normal and cirrhotic rat liver: implications for regulation of portal pressure and resistance. Hepatology 1996;24:233-40. - PubMed
-
- Wiest R, Groszmann RJ. The paradox of nitric oxide in cirrhosis and portal hypertension: too much, not enough. Hepatology 2002;35:478-91. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources