

Markers of exacerbation severity in chronic obstructive pulmonary disease
- PMID: 16686949
- PMCID: PMC1481583
- DOI: 10.1186/1465-9921-7-74
Markers of exacerbation severity in chronic obstructive pulmonary disease
Abstract
Background: Patients with chronic obstructive pulmonary disease (COPD) can experience 'exacerbations' of their conditions. An exacerbation is an event defined in terms of subjective descriptors or symptoms, namely dyspnoea, cough and sputum that worsen sufficiently to warrant a change in medical management. There is a need for reliable markers that reflect the pathological mechanisms that underlie exacerbation severity and that can be used as a surrogate to assess treatment effects in clinical studies. Little is known as to how existing study variables and suggested markers change in both the stable and exacerbation phases of COPD. In an attempt to find the best surrogates for exacerbations, we have reviewed the literature to identify which of these markers change in a consistent manner with the severity of the exacerbation event.
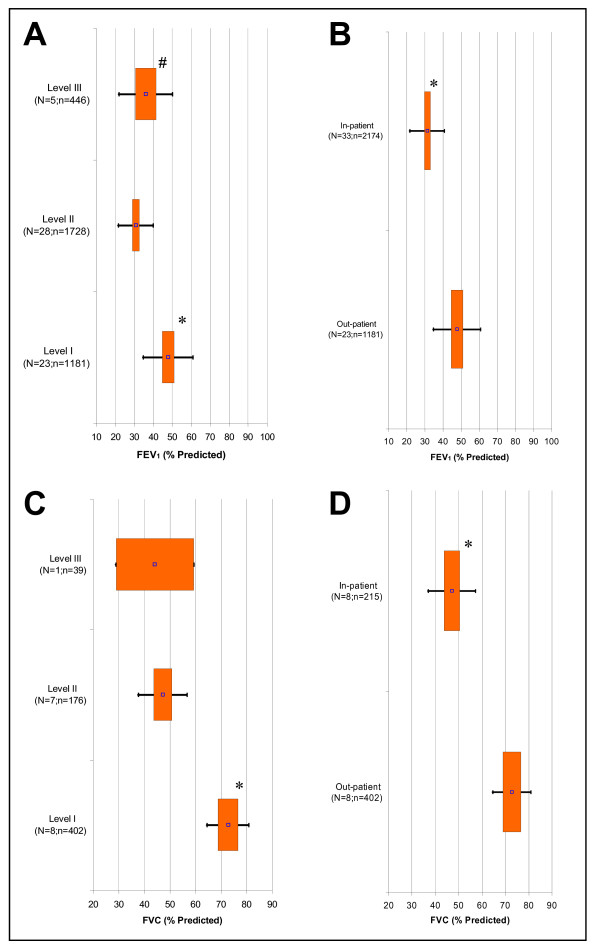
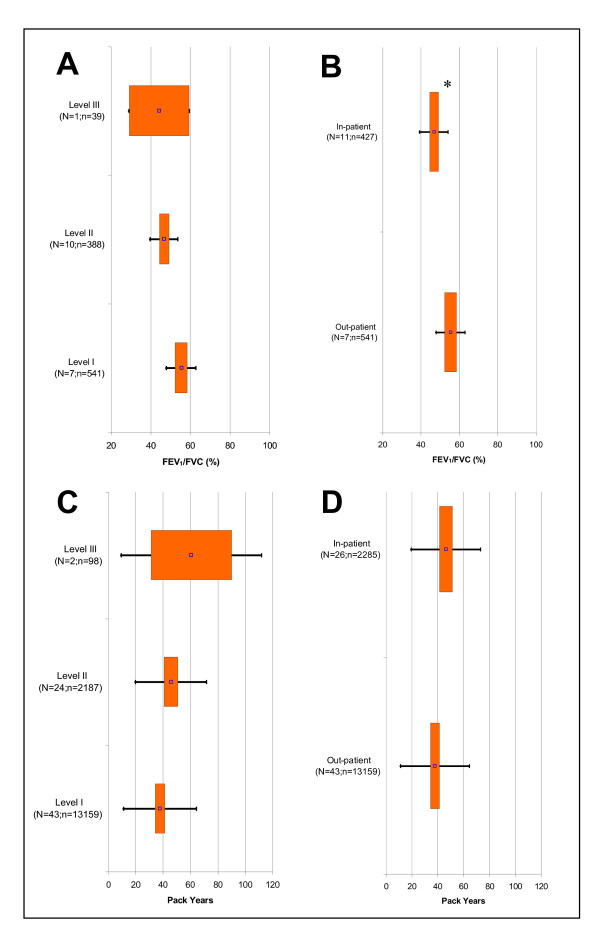
Methods: We have searched standard databases between 1966 to July 2004 using major keywords and terms. Studies that provided demographics, spirometry, potential markers, and clear eligibility criteria were included in this study. Central tendencies and dispersions for all the variables and markers reported and collected by us were first tabulated according to sample size and ATS/ERS 2004 Exacerbation Severity Levels I to III criteria. Due to the possible similarity of patients in Levels II and III, the data was also redefined into categories of exacerbations, namely out-patient (Level I) and in-patient (Levels II & III combined). For both approaches, we performed a fixed effect meta-analysis on each of the reported variables.
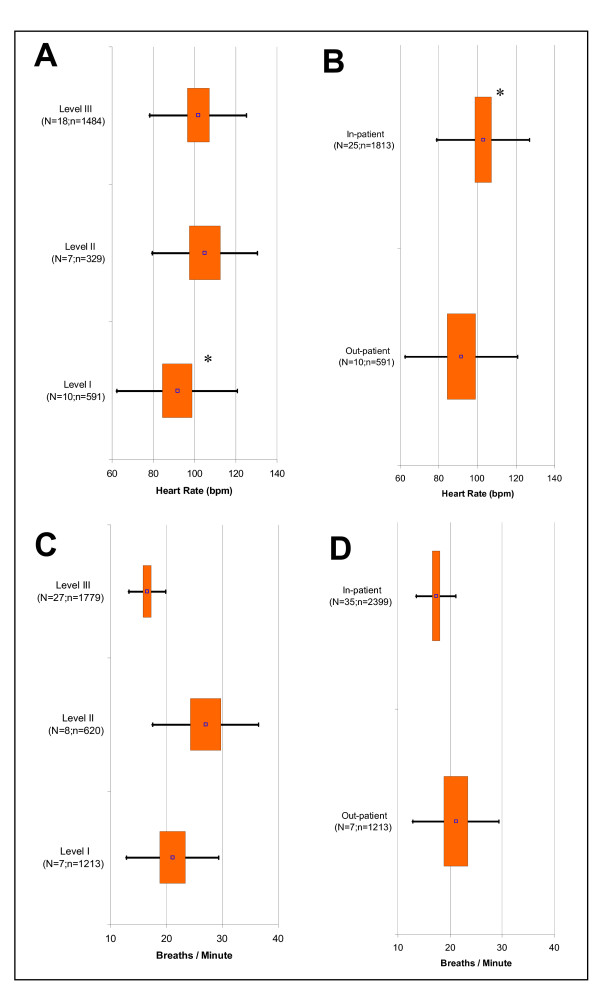
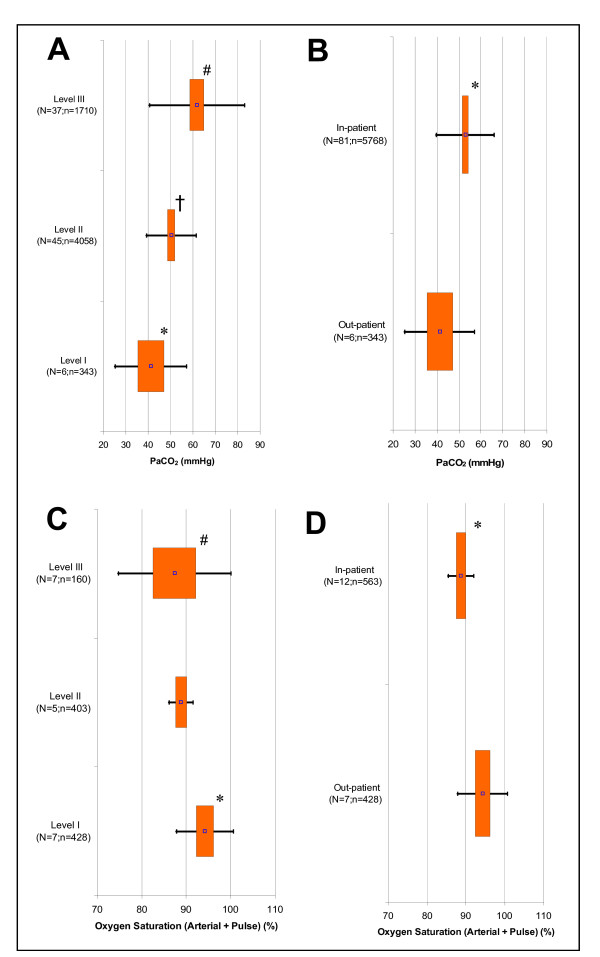
Results: We included a total of 268 studies reported between 1979 to July 2004. These studies investigated 142,407 patients with COPD. Arterial carbon dioxide tension and breathing rate were statistically different between all levels of exacerbation severity and between in out- and in-patient settings. Most other measures showed weak relationships with either level or setting, or they had insufficient data to permit meta-analysis.
Conclusion: Arterial carbon dioxide and breathing rate varied in a consistent manner with exacerbation severity and patient setting. Many other measures showed weak correlations that should be further explored in future longitudinal studies or assessed using suggested mathematical modelling techniques.
Figures
References
-
- Celli BR, MacNee W. Standards for the diagnosis and treatment of patients with COPD: a summary of the ATS/ERS position paper. Eur Respir J. 2004;23:932–946. - PubMed
-
- Wedzicha JA, Donaldson GC. Exacerbations of chronic obstructive pulmonary disease. Respir Care. 2003;48:1204–1213. - PubMed
-
- Seemungal TA, Donaldson GC, Paul EA, Bestall JC, Jeffries DJ, Wedzicha JA. Effect of exacerbation on quality of life in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157:1418–1422. - PubMed
-
- Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106:196–204. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
