

Primary intracranial atypical teratoid/rhabdoid tumors of infancy and childhood: MRI features and patient outcomes
- PMID: 16687525
- PMCID: PMC7975730
Primary intracranial atypical teratoid/rhabdoid tumors of infancy and childhood: MRI features and patient outcomes
Abstract
Background and purpose: Primary atypical teratoid/rhabdoid tumors (AT/RTs) are rare malignant intracranial neoplasms, usually occurring in young children. The objectives of this study were to characterize the MR imaging features and locations of primary intracranial AT/RTs, to determine the frequency of disseminated disease in the central nervous system (CNS) at diagnosis and postoperatively, and to assess patient outcomes.
Methods: The preoperative cranial MR images of 13 patients with AT/RTs were retrospectively reviewed for evaluation of lesion location, size, MR signal intensity and enhancement characteristics, and the presence of disseminated intracranial tumor. Postoperative MR images of the head and spine for 17 patients were reviewed for the presence of locally recurrent or residual tumor and disseminated neoplasm. Imaging data were correlated with patient outcomes.
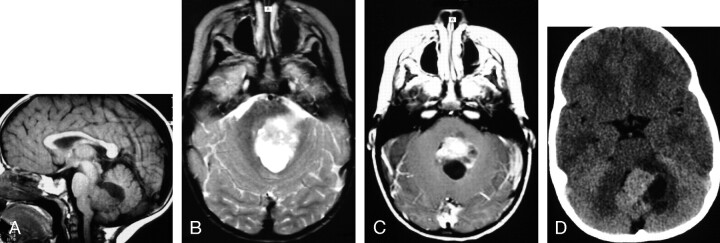
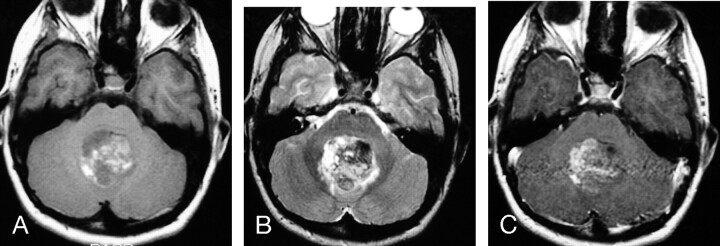
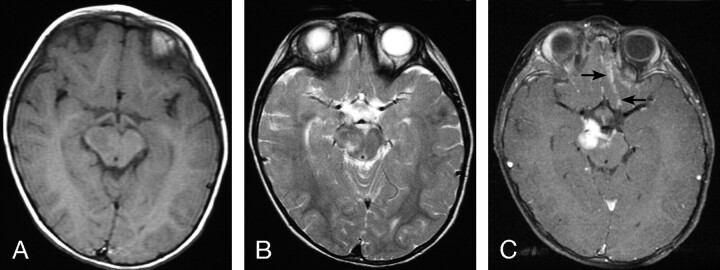
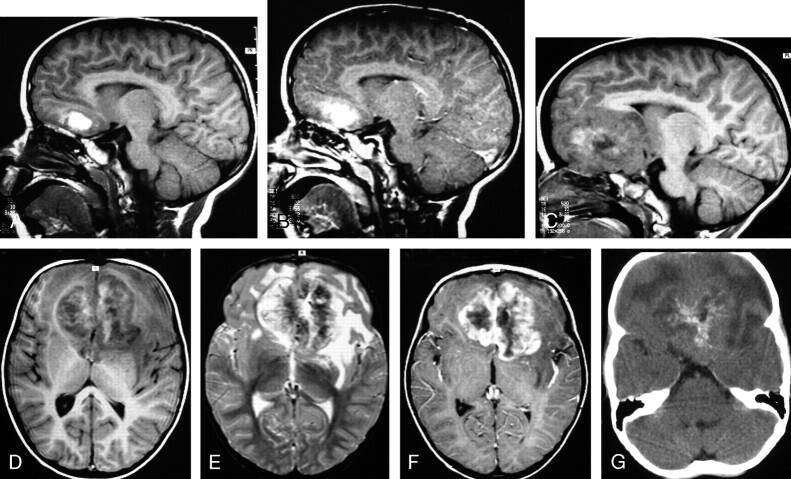
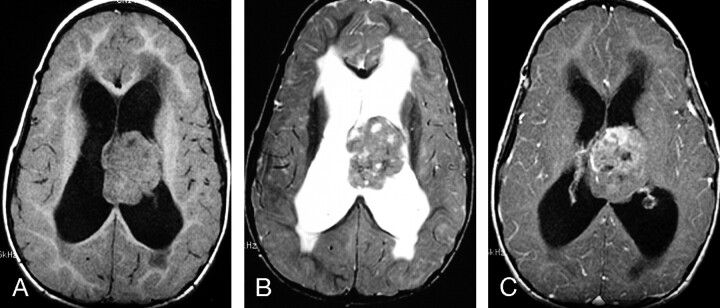
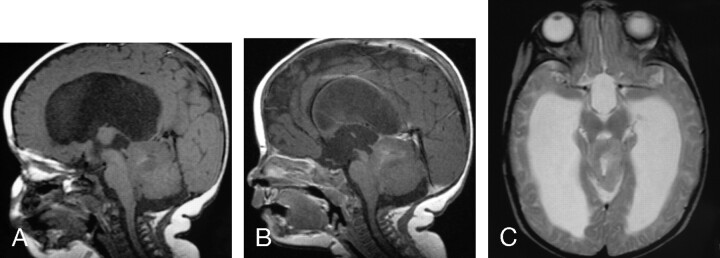
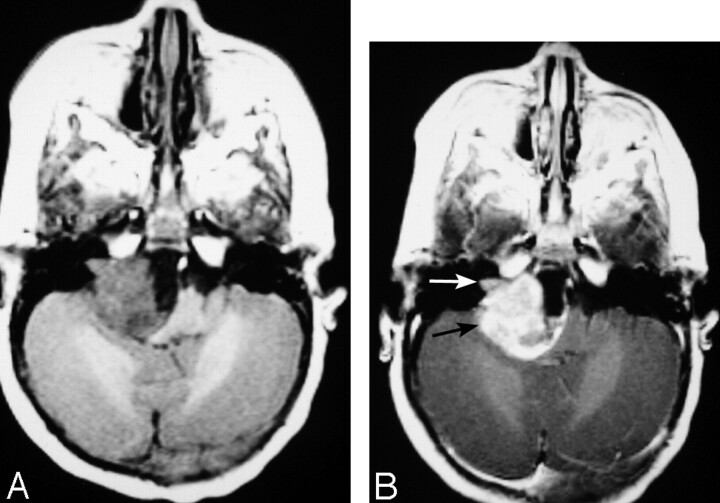
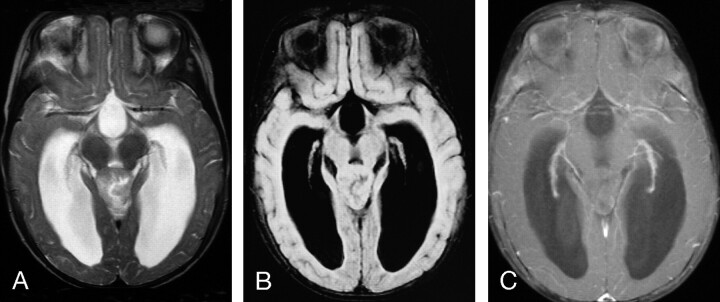
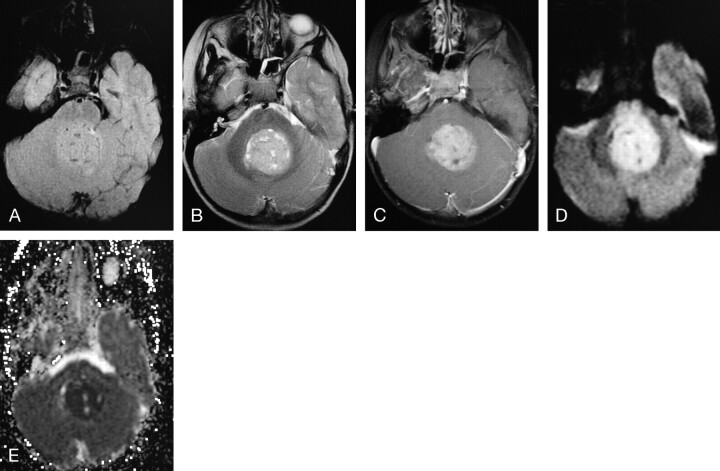
Results: Patients ranged in age from 4 months to 15 years (median age, 2.9 years). Primary AT/RTs were intra-axial in 94% of patients. The single primary extra-axial lesion was located in the cerebellopontine angle cistern. AT/RTs were infratentorial in 47%, supratentorial in 41%, and both infra- and supratentorial in 12%. A germ-line mutation of the hSNF5/INI1 tumor-suppressor gene was responsible for the simultaneous occurrence of an intracranial AT/RT and a malignant renal rhabdoid tumor in a 4-month-old patient. Mean tumor sizes were 3.6 x 3.8 x 3.9 cm. On short TR images, AT/RTs typically had heterogeneous intermediate signal intensity, as well as zones of low (54%), high (8%), or both low and high (31%) signal intensity from cystic and/or necrotic regions, hemorrhage, or both, respectively. On long TR/long TE images, solid portions of AT/RTs typically had heterogeneous intermediate-to-slightly-high signal intensity with additional zones of high (54%) or both high and low signal intensity (38%), secondary to cystic and/or necrotic regions, edema, prior hemorrhage, and/or calcifications. AT/RT had isointense and/or slightly hyperintense signal intensity relative to gray matter on fluid-attenuated inversion-recovery (FLAIR) and long TR/long TE images, and showed restricted diffusion. All except 1 AT/RT showed contrast enhancement. The fraction of tumor volume showing enhancement was greater than two thirds in 58%, between one third and two thirds in 33%, and less than one third in 9%. Disseminated tumor in the leptomeninges was seen with MR imaging in 24% of patients at diagnosis/initial staging and occurred in another 35% from 4 months to 2.8 years (mean, 1.1 years) after surgery and earlier imaging examinations with negative findings. The overall 1-year and 5-year survival probabilities were 71% and 28%, respectively. Patients with MR imaging evidence of disseminated leptomeningeal tumor had a median survival rate of 16 months compared with 149 months for those without disseminated tumor (P < .004, logrank test).
Conclusion: AT/RTs are typically intra-axial lesions, which can be infra- and/or supratentorial. The unenhanced and enhanced MR imaging features of AT/RT are often variable secondary to cystic/necrotic changes, hemorrhage, and/or calcifications. Poor prognosis is associated with MR imaging evidence of disseminated leptomeningeal tumor.
Figures
Similar articles
-
Choroid plexus carcinomas in children: MRI features and patient outcomes.Neuroradiology. 2004 Sep;46(9):770-80. doi: 10.1007/s00234-004-1238-7. Neuroradiology. 2004. PMID: 15309348
-
MRI features of atypical teratoid/rhabdoid tumors in children.Pediatr Radiol. 2013 Aug;43(8):1001-8. doi: 10.1007/s00247-013-2646-9. Epub 2013 Mar 7. Pediatr Radiol. 2013. PMID: 23467756
-
Imaging findings in primary intracranial atypical teratoid/rhabdoid tumors.Pediatr Radiol. 2006 Feb;36(2):126-32. doi: 10.1007/s00247-005-0037-6. Epub 2005 Dec 8. Pediatr Radiol. 2006. PMID: 16341528
-
Central nervous system atypical teratoid/rhabdoid tumors of infancy and childhood.Ultrastruct Pathol. 1997 Jul-Aug;21(4):369-78. doi: 10.3109/01913129709021935. Ultrastruct Pathol. 1997. PMID: 9206002 Review.
-
Spinal atypical teratoid rhabdoid tumor-narrative review and report of a rare case managed with multimodality approach.Childs Nerv Syst. 2023 Aug;39(8):2019-2026. doi: 10.1007/s00381-023-05977-2. Epub 2023 May 9. Childs Nerv Syst. 2023. PMID: 37160436 Review.
Cited by
-
Radiomic Phenotypes Distinguish Atypical Teratoid/Rhabdoid Tumors from Medulloblastoma.AJNR Am J Neuroradiol. 2021 Sep;42(9):1702-1708. doi: 10.3174/ajnr.A7200. Epub 2021 Jul 15. AJNR Am J Neuroradiol. 2021. PMID: 34266866 Free PMC article.
-
Neuroimaging of pediatric tumors of the sellar region-A review in light of the 2021 WHO classification of tumors of the central nervous system.Front Pediatr. 2023 Jun 21;11:1162654. doi: 10.3389/fped.2023.1162654. eCollection 2023. Front Pediatr. 2023. PMID: 37416813 Free PMC article. Review.
-
A Systematic Review of Atypical Teratoid Rhabdoid Tumor in Adults.Front Oncol. 2018 Nov 28;8:567. doi: 10.3389/fonc.2018.00567. eCollection 2018. Front Oncol. 2018. PMID: 30547013 Free PMC article.
-
Deciphering Machine Learning Decisions to Distinguish between Posterior Fossa Tumor Types Using MRI Features: What Do the Data Tell Us?Cancers (Basel). 2023 Aug 8;15(16):4015. doi: 10.3390/cancers15164015. Cancers (Basel). 2023. PMID: 37627043 Free PMC article.
-
Multimodal treatments combined with gamma knife surgery for primary atypical teratoid/rhabdoid tumor of the central nervous system: a single-institute experience of 18 patients.Childs Nerv Syst. 2018 Apr;34(4):627-638. doi: 10.1007/s00381-017-3688-3. Epub 2017 Dec 7. Childs Nerv Syst. 2018. PMID: 29218405
References
-
- Burger PC, Yu I-T, Friedman HS, et al. Atypical teratoid/rhabdoid tumor of the central nervous system: a highly malignant tumor of infancy and childhood frequently mistaken for medulloblastoma—a pediatric oncology study. Am J Surg Pathol 1998;22:1083–92 - PubMed
-
- Rickert CH, Paulus W. Epidemiology of central nervous system tumors in childhood and adolescence based on the new WHO classification. Childs Nerv Syst 2001;17:503–11 - PubMed
-
- Rorke LB, Packer RJ, Biegel JA. Central nervous system atypical teratoid/rhabdoid tumors of infancy and childhood: definition of an entity. J Neurosurg 1996;85:56–65 - PubMed
-
- Biegel JA, Fogelgren B, Zhou JY, et al. Mutations of the INI1 rhabdoid tumor suppressor gene in medulloblastomas and primitive neuroectodermal tumors of the central nervous system. Clin Cancer Res 2000;6:2759–63 - PubMed
-
- Bruch LA, Hill A, Cai DX, et al. A role for fluorescence in situ hybridization detection for chromosome 22q dosage in distinguishing atypical teratoid/rhabdoid tumors from medulloblastoma/central primitive neuroectodermal tumors. Hum Pathol 2001;32:156–62 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical