

Serial testing of health care workers for tuberculosis using interferon-gamma assay
- PMID: 16690977
- PMCID: PMC2648116
- DOI: 10.1164/rccm.200604-472OC
Serial testing of health care workers for tuberculosis using interferon-gamma assay
Abstract
Rationale: Although interferon-gamma (IFN-gamma) assays are promising alternatives to the tuberculin skin test (TST), their serial testing performance is unknown.
Objective: To compare TST and IFN-gamma conversions and reversions in healthcare workers.
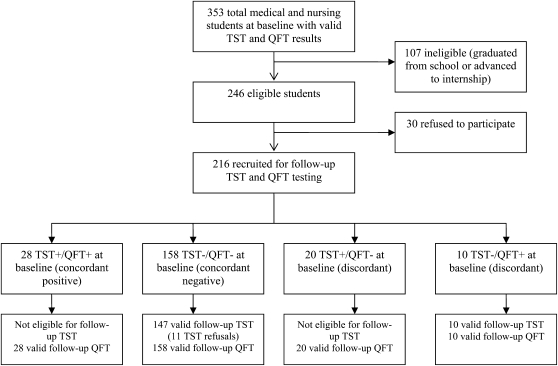
Methods: We prospectively followed-up 216 medical and nursing students in India who underwent baseline and repeat testing (after 18 mo) with TST and QuantiFERON-TB Gold In-Tube (QFT). TST conversions were defined as reactions greater than or equal to 10 mm, with increments of 6 or 10 mm over baseline. QFT conversions were defined as baseline IFN-gamma less than 0.35 and follow-up IFN-gamma greater than or equal to 0.35 or 0.70 IU/ml. QFT reversions were defined as baseline IFN-gamma greater than or equal to 0.35 and follow-up IFN-gamma less than 0.35 IU/ml.
Results: Of the 216 participants, 48 (22%) were TST-positive, and 38 (18%) were QFT-positive at baseline. Among 147 participants with concordant baseline negative results, TST conversions occurred in 14 (9.5%; 95% confidence interval [CI] = 5.3-15.5) using the 6 mm increment definition, and 6 (4.1%; 95% CI = 1.5-8.7) using the 10 mm increment definition. QFT conversions occurred in 17/147 participants (11.6%; 95% CI = 6.9-17.9) using the definition of IFN-gamma greater than or equal to 0.35 IU/ml, and 11/147 participants (7.5%; 95% CI = 3.8-13.0) using IFN-gamma greater than or equal to 0.70 IU/ml. Agreement between TST (10 mm increment) and QFT conversions (>or= 0.70 IU/ml) was 96% (kappa = 0.70). QFT reversions occurred in 2/28 participants (7%) with baseline concordant positive results, as compared with 7/10 participants (70%) with baseline discordant results (p < 0.001).
Conclusions: IFN-gamma assay shows promise for serial testing, but repeat results need to be interpreted carefully. To meaningfully interpret serial results, the optimal thresholds to distinguish new infections from nonspecific variations must be determined.
Figures
References
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, Raviglione MC, Dye C. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med 2003;163:1009–1021. - PubMed
-
- World Health Organization. Global Tuberculosis Control. Surveillance, Planning, Financing: WHO Report 2005. Geneva: World Health Organization; 2005. pp. 1–247.
-
- Menzies D, Fanning A, Yuan L, Fitzgerald M. Tuberculosis among health care workers. N Engl J Med 1995;332:92–98. - PubMed
-
- Blumberg HM. 2004. Tuberculosis infection control in healthcare settings. In: Lautenbach E, Woeltje K, editors. Practical handbook for healthcare epidemiologists. Thorofare, NJ: Slack Incorporated. pp. 259–273.
-
- Centers for Disease Control and Prevention. Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR 2005;54:1–141. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical