

Non alcoholic fatty liver disease: a clinical approach and review
- PMID: 16691301
- PMCID: PMC2659893
- DOI: 10.1155/2006/918262
Non alcoholic fatty liver disease: a clinical approach and review
Abstract
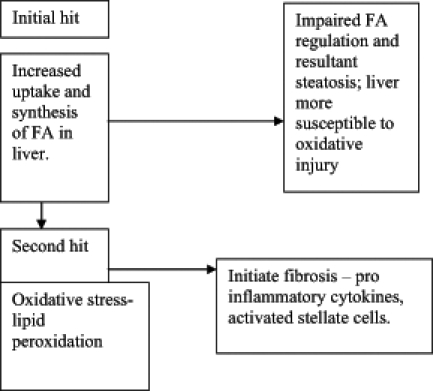
Nonalcoholic fatty liver disease (NAFLD) is the most common cause of incidental elevation of liver enzymes in North America and Europe. Risk factors for NAFLD include body mass index of 25 kg/m2 or greater, central obesity and diabetes mellitus. The spectrum of disease is variable, ranging from simple steatosis with benign prognosis, to non-alcoholic steatohepatitis and cirrhosis, conferring increase in morbidity and mortality. The primary abnormality or 'first hit' in patients with NAFLD is insulin resistance leading to hepatic steatosis. The second hit involves multiple proinflammatory cytokines resulting in non-alcoholic steatohepatitis. Treatment is aimed at aggressive risk factor control and weight loss. Currently, there are no pharmacological agents recommended in the treatment of NAFLD, although preliminary studies suggest promising agents in the future.
La stéatose hépatique non alcoolique (SHNA) est la principale cause d’élévation auxiliaire des enzymes hépatiques en Amérique du Nord et en Europe. Les facteurs de risque de SHNA incluent un indice de masse corporelle de 25 kg/m2 ou une obésité tronculaire encore plus importante accompagnée d’un diabète sucré. Le spectre de la maladie est variable, d’une stéatose simple au pronostic bénin à une stéatohépatite non alcoolique associée à une cirrhose qui augmente la morbidité et la mortalité. L’anomalie primaire, ou première occurrence, chez les patients atteints d’une SHNA est une insulinorésistance provoquant une stéatohépatite. La deuxième occurrence touche des cytokines pro-inflammatoires multiples entraînant une stéatohépatite non alcoolique. Le traitement vise le contrôle agressif des facteurs de risque et la perte de poids. Pour l’instant, aucun agent pharmacologique n’est recommandé pour traiter la SHNA, mais des études préliminaires sont prometteuses à cet égard.
Figures
References
-
- Ludwig J, Viggiano TR, McGill DB, Ott BJ. Nonalcoholic steatohepatitis. Mayo Clin Proc. 1980;55:434–8. - PubMed
-
- Mezey E. Dietary fat and alcoholic liver disease. Hepatology. 1998;28:901–5. - PubMed
-
- Bellantani S, Saccoccio G, Masutti F, et al. Prevalence of and risk factors for hepatic steatosis in northern Italy. Ann Intern Med. 2000;132:112–7. - PubMed
-
- Gupte P, Amarapurkar D, Agal S, et al. Nonalcoholic steatohepatitis in type 2 diabetes mellitus. J Gastroenterol Hepatol. 2004;19:854–8. - PubMed
-
- Lee JH, Rhee PL, Lee JK, et al. Role of hyperinsulinemia and glucose intolerance in the pathogenesis of nonalcoholic fatty liver in patients with normal body weight. Korean J Intern Med. 1998;13:12–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical