

RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis
- PMID: 16696865
- PMCID: PMC1550961
- DOI: 10.1186/cc4915
RIFLE criteria for acute kidney injury are associated with hospital mortality in critically ill patients: a cohort analysis
Abstract
Introduction: The lack of a standard definition for acute kidney injury has resulted in a large variation in the reported incidence and associated mortality. RIFLE, a newly developed international consensus classification for acute kidney injury, defines three grades of severity--risk (class R), injury (class I) and failure (class F)--but has not yet been evaluated in a clinical series.
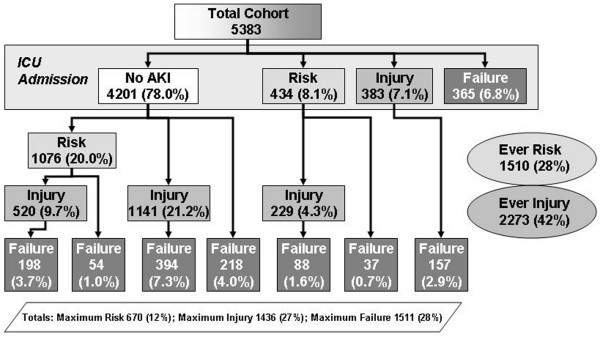
Methods: We performed a retrospective cohort study, in seven intensive care units in a single tertiary care academic center, on 5,383 patients admitted during a one year period (1 July 2000-30 June 2001).
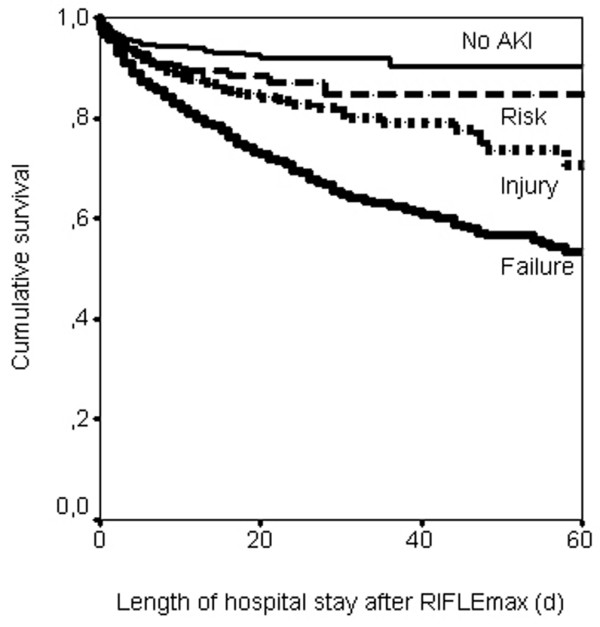
Results: Acute kidney injury occurred in 67% of intensive care unit admissions, with maximum RIFLE class R, class I and class F in 12%, 27% and 28%, respectively. Of the 1,510 patients (28%) that reached a level of risk, 840 (56%) progressed. Patients with maximum RIFLE class R, class I and class F had hospital mortality rates of 8.8%, 11.4% and 26.3%, respectively, compared with 5.5% for patients without acute kidney injury. Additionally, acute kidney injury (hazard ratio, 1.7; 95% confidence interval, 1.28-2.13; P < 0.001) and maximum RIFLE class I (hazard ratio, 1.4; 95% confidence interval, 1.02-1.88; P = 0.037) and class F (hazard ratio, 2.7; 95% confidence interval, 2.03-3.55; P < 0.001) were associated with hospital mortality after adjusting for multiple covariates.
Conclusion: In this general intensive care unit population, acute kidney 'risk, injury, failure', as defined by the newly developed RIFLE classification, is associated with increased hospital mortality and resource use. Patients with RIFLE class R are indeed at high risk of progression to class I or class F. Patients with RIFLE class I or class F incur a significantly increased length of stay and an increased risk of inhospital mortality compared with those who do not progress past class R or those who never develop acute kidney injury, even after adjusting for baseline severity of illness, case mix, race, gender and age.
Figures
References
-
- Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, Sirio CA, Murphy DJ, Lotring T, Damiano A, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991;100:1619–1636. - PubMed
-
- Vincent J-L, Moreno R, Takala J, Willatts S, de Mendonça A, Bruining H, Reinhart CK, Suter PeterM, Thijs LG. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996;22:707–710. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
