

Impact of specialty of admitting physician and type of hospital on care and outcome for myocardial infarction in England and Wales during 2004-5: observational study
- PMID: 16705004
- PMCID: PMC1473062
- DOI: 10.1136/bmj.38849.440914.AE
Impact of specialty of admitting physician and type of hospital on care and outcome for myocardial infarction in England and Wales during 2004-5: observational study
Abstract
Objective: To examine process of care and outcome for patients admitted with acute myocardial infarction to hospitals in England and Wales in relation to type of consultant care and type of hospital.
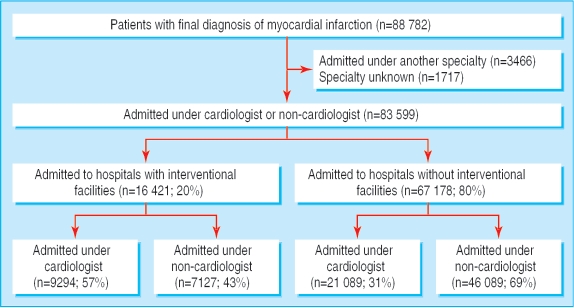
Design: Observational study of 88,782 patients admitted with myocardial infarction during 2004-5, using records from the national audit of myocardial infarction project (MINAP) database.
Outcome measures: Use of reperfusion treatment and secondary prevention drugs, use of angiography, and 90 day mortality of patients admitted under the care of cardiologists and non-cardiologists in hospitals with and without facilities for coronary intervention.
Findings: 36% of patients were admitted under the care of a cardiologist and 20% to a hospital with coronary interventional facilities. Patients admitted under cardiologists had fewer comorbidities than other patients and were more likely to have reperfusion treatment (12,266/14,433 (85%) v 13,682/17,064 (80%)) and appropriate secondary prevention drugs. Overall, 27,431/79,374 (35%) of patients had angiography. Relatively more patients admitted to interventional hospitals (8167/14,661; 56%) than to other hospitals had angiography (19,264/64,713; 30%). The adjusted risk of death by 90 days for patients treated in interventional compared with non-interventional hospitals was 0.93 (95% confidence interval 0.82 to 1.06). The adjusted risk of death at 90 days for patients admitted under cardiologists compared with non-cardiologists was 0.86 (0.81 to 0.91).
Conclusions: Patients cared for by cardiologists had less comorbidity than other patients. They were more likely to receive proved treatments and angiography, and they had a lower adjusted 90 day mortality. Large differences existed in the use of angiography between interventional and non-interventional hospitals. These findings show wide variations in the management and outcome of patients with myocardial infarction in England and Wales.
References
-
- Block P, Weber H, Kearney P, Cardiology Section of the European Union of Medical Specialists. Manpower in cardiology II in western and central Europe (1999-2000). Eur Heart J 2003;24: 299-310. - PubMed
-
- Birkhead JS, Georgiou A, Knight L, Walker L, Lowe D, eds. A baseline survey of facilities for the management of acute myocardial infarction in England 2000. London: Royal College of Physicians, 2001.
-
- Birkhead JS, Pearson M, Norris RM, Rickards AF, Georgiou A. The national audit of myocardial infarction: a new development in the audit process. Journal of Clinical Excellence 2002;4: 379-85.
-
- Royal College of Physicians. MINAP data set. www.rcplondon.ac.uk/college/ceeu/ceeu_ami_home.htm (accessed 24 Dec 2005).
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical