

Lung adenocarcinomas induced in mice by mutant EGF receptors found in human lung cancers respond to a tyrosine kinase inhibitor or to down-regulation of the receptors
- PMID: 16705038
- PMCID: PMC1475762
- DOI: 10.1101/gad.1417406
Lung adenocarcinomas induced in mice by mutant EGF receptors found in human lung cancers respond to a tyrosine kinase inhibitor or to down-regulation of the receptors
Abstract
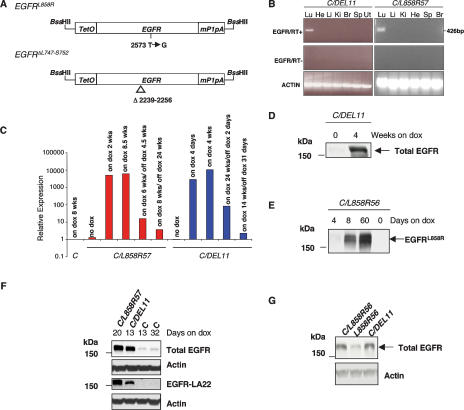
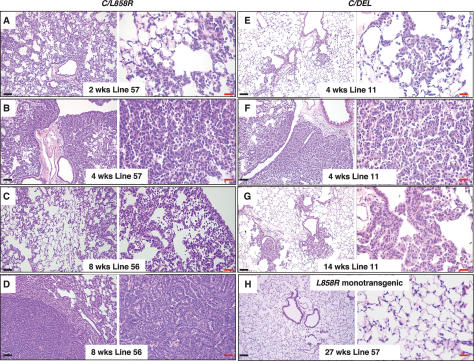
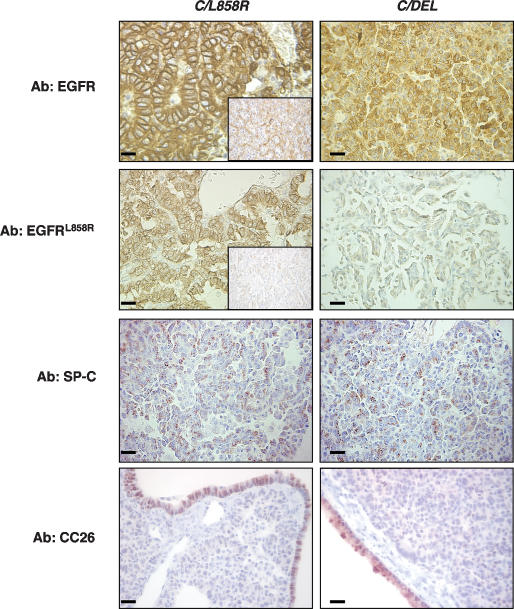
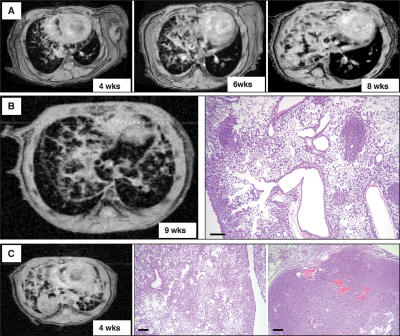
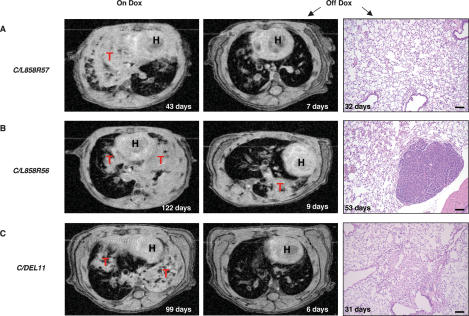
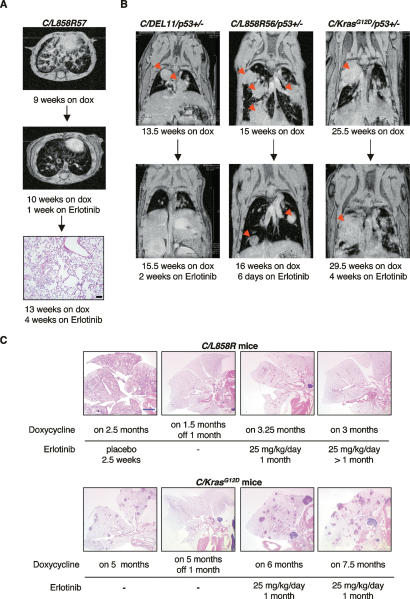
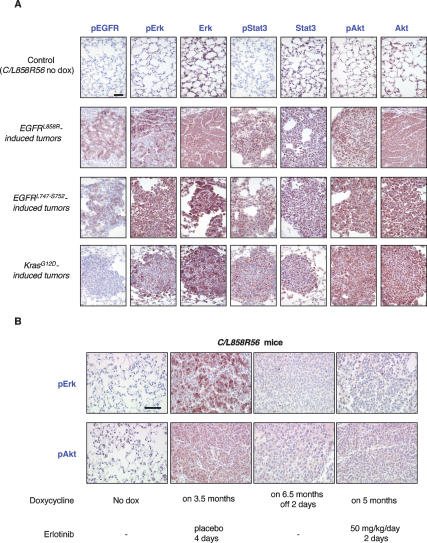
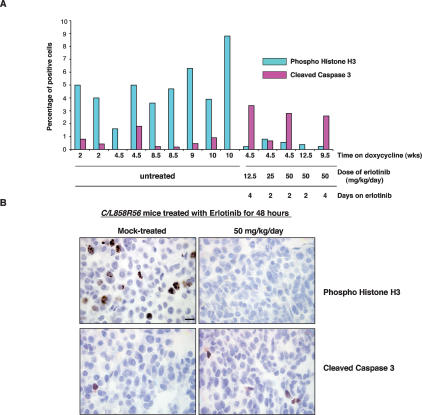
Somatic mutations in exons encoding the tyrosine kinase domain of the epidermal growth factor receptor (EGFR) gene are found in human lung adenocarcinomas and are associated with sensitivity to the tyrosine kinase inhibitors gefitinib and erlotinib. Nearly 90% of the EGFR mutations are either short, in-frame deletions in exon 19 or point mutations that result in substitution of arginine for leucine at amino acid 858 (L858R). To study further the role of these mutations in the initiation and maintenance of lung cancer, we have developed transgenic mice that express an exon 19 deletion mutant (EGFR(DeltaL747-S752)) or the L858R mutant (EGFR(L858R)) in type II pneumocytes under the control of doxycycline. Expression of either EGFR mutant leads to the development of lung adenocarcinomas. Two weeks after induction with doxycycline, mice that express the EGFR(L858R) allele show diffuse lung cancer highly reminiscent of human bronchioloalveolar carcinoma and later develop interspersed multifocal adenocarcinomas. In contrast, mice expressing EGFR(DeltaL747-S752) develop multifocal tumors embedded in normal lung parenchyma with a longer latency. With mice carrying either EGFR allele, withdrawal of doxycycline (to reduce expression of the transgene) or treatment with erlotinib (to inhibit kinase activity) causes rapid tumor regression, as assessed by magnetic resonance imaging and histopathology, demonstrating that mutant EGFR is required for tumor maintenance. These models may be useful for developing improved therapies for patients with lung cancers bearing EGFR mutations.
Figures
References
-
- Amann J., Kalyankrishna S., Massion P.P., Ohm J.E., Girard L., Shigematsu H., Peyton M., Juroske D., Huang Y., Stuart Salmon J., et al. Aberrant epidermal growth factor receptor signaling and enhanced sensitivity to EGFR inhibitors in lung cancer. Cancer Res. 2005;65:226–235. - PubMed
-
- Barkley J.E., Green M.R. Bronchioloalveolar carcinoma. J. Clin. Oncol. 1996;14:2377–2386. - PubMed
-
- Boxer R.B., Jang J.W., Sintasath L., Chodosh L.A. Lack of sustained regression of c-MYC-induced mammary adenocarcinomas following brief or prolonged MYC inactivation. Cancer Cell. 2004;6:577–586. - PubMed
-
- Cappuzzo F., Hirsch F.R., Rossi E., Bartolini S., Ceresoli G.L., Bemis L., Haney J., Witta S., Danenberg K., Domenichini I., et al. Epidermal growth factor receptor gene and protein and gefitinib sensitivity in non-small-cell lung cancer. J. Natl. Cancer Inst. 2005;97:643–655. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous