

Heart failure, chronic diuretic use, and increase in mortality and hospitalization: an observational study using propensity score methods
- PMID: 16709595
- PMCID: PMC2443408
- DOI: 10.1093/eurheartj/ehi890
Heart failure, chronic diuretic use, and increase in mortality and hospitalization: an observational study using propensity score methods
Abstract
Aims: Non-potassium-sparing diuretics are commonly used in heart failure (HF). They activate the neurohormonal system, and are potentially harmful. Yet, the long-term effects of chronic diuretic use in HF are largely unknown. We retrospectively analysed the Digitalis Investigation Group (DIG) data to determine the effects of diuretics on HF outcomes.
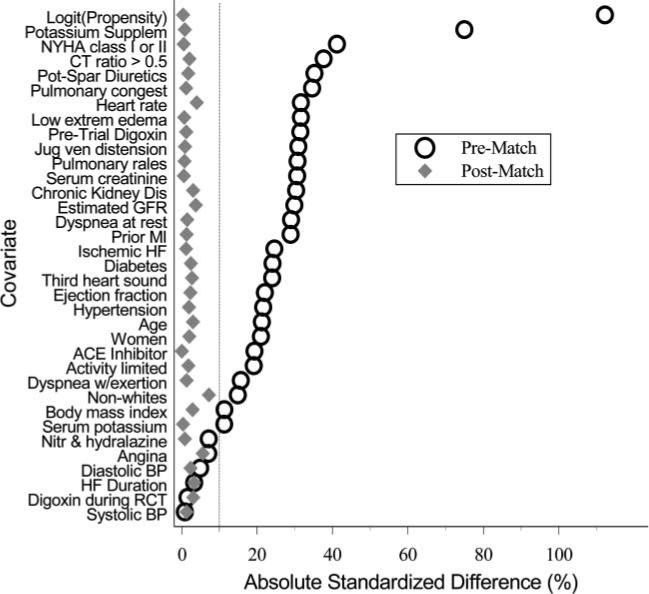
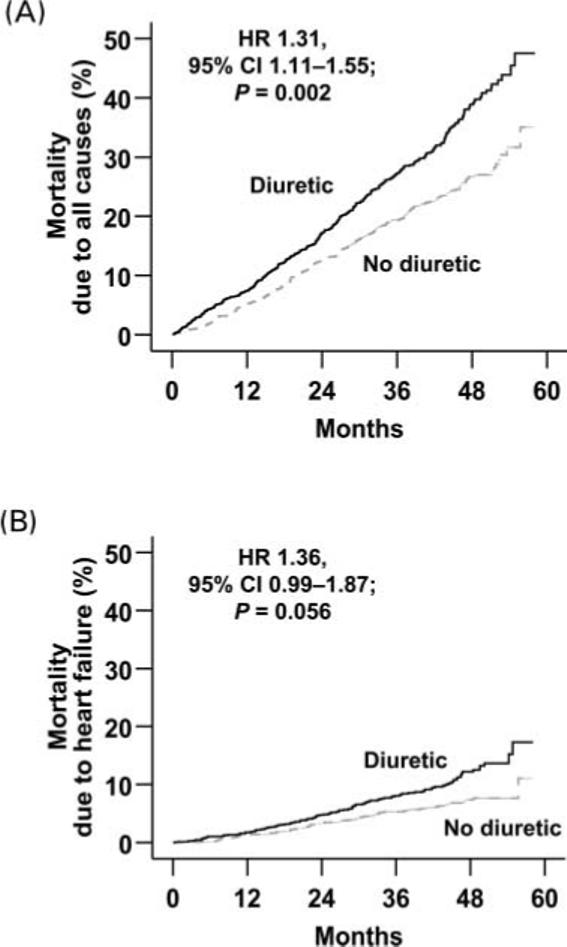
Methods and results: Propensity scores for diuretic use were calculated for each of the 7788 DIG participants using a non-parsimonious multivariable logistic regression model, and were used to match 1391 (81%) no-diuretic patients with 1391 diuretic patients. Effects of diuretics on mortality and hospitalization at 40 months of median follow-up were assessed using matched Cox regression models. All-cause mortality was 21% for no-diuretic patients and 29% for diuretic patients [hazard ratio (HR) 1.31; 95% confidence interval (CI) 1.11-1.55; P = 0.002]. HF hospitalizations occurred in 18% of no-diuretic patients and 23% of diuretic patients (HR 1.37; 95% CI 1.13-1.65; P = 0.001).
Conclusion: Chronic diuretic use was associated with increased long-term mortality and hospitalizations in a wide spectrum of ambulatory chronic systolic and diastolic HF patients. The findings of the current study challenge the wisdom of routine chronic use of diuretics in HF patients who are asymptomatic or minimally symptomatic without fluid retention, and are on complete neurohormonal blockade. These findings, based on a non-randomized design, need to be further studied in randomized trials.
Figures


References
-
- Hunt SA, Abraham WT, Chin MH, Feldman AM, Francis GS, Ganiats TG, Jessup M, Konstam MA, Mancini DM, Michl K, Oates JA, Rahko PS, Silver MA, Stevenson LW, Yancy CW, Antman EM, Smith SC, Jr, Adams CD, Anderson JL, Faxon DP, Fuster V, Halperin JL, Hiratzka LF, Jacobs AK, Nishimura R, Ornato JP. ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Update the 2001 Guidelines for the Evaluation and Management of Heart Failure). Developed in Collaboration With the American College of Chest Physicians and the International Society for Heart and Lung Transplantation. Endorsed by the Heart Rhythm Society. Circulation. 2005;112:e154–e235. Published online before print September 13, 2005, doi:10.1161/CIRCULATIONAHA.105.167586. - PubMed
-
- Swedberg K, Cleland J, Dargie H, Drexler H, Follath F, Komajda M, Tavazzi L, Smiseth OA, Gavazzi A, Haverich A, Hoes A, Jaarsma T, Korewicki J, Levy S, Linde C, Lopez-Sendon JL, Nieminen MS, Pierard L, Remme WJ. Guidelines for the diagnosis and treatment of chronic heart failure: executive summary (update 2005): The Task Force for the Diagnosis and Treatment of Chronic Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:1115–1140. - PubMed
-
- Francis GS, Siegel RM, Goldsmith SR, Olivari MT, Levine TB, Cohn JN. Acute vasoconstrictor response to intravenous furosemide in patients with chronic congestive heart failure. Activation of the neurohumoral axis. Ann Intern Med. 1985;103:1–6. - PubMed
-
- Francis GS, Benedict C, Johnstone DE, Kirlin PC, Nicklas J, Liang CS, Kubo SH, Rudin-Toretsky E, Yusuf S. Comparison of neuroendocrine activation in patients with left ventricular dysfunction with and without congestive heart failure. A substudy of the Studies of Left Ventricular Dysfunction (SOLVD). Circulation. 1990;82:1724–1729. - PubMed
-
- Sigurdsson A, Swedberg K. Neurohormonal activation and congestive heart failure: today's experience with ACE inhibitors and rationale for their use. Eur Heart J. 1995;16(Suppl N):65–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
