

Monthly intravenous methylprednisolone in relapsing-remitting multiple sclerosis - reduction of enhancing lesions, T2 lesion volume and plasma prolactin concentrations
- PMID: 16719908
- PMCID: PMC1501038
- DOI: 10.1186/1471-2377-6-19
Monthly intravenous methylprednisolone in relapsing-remitting multiple sclerosis - reduction of enhancing lesions, T2 lesion volume and plasma prolactin concentrations
Abstract
Background: Intravenous methylprednisolone (IV-MP) is an established treatment for multiple sclerosis (MS) relapses, accompanied by rapid, though transient reduction of gadolinium enhancing (Gd+) lesions on brain MRI. Intermittent IV-MP, alone or with immunomodulators, has been suggested but insufficiently studied as a strategy to prevent relapses.
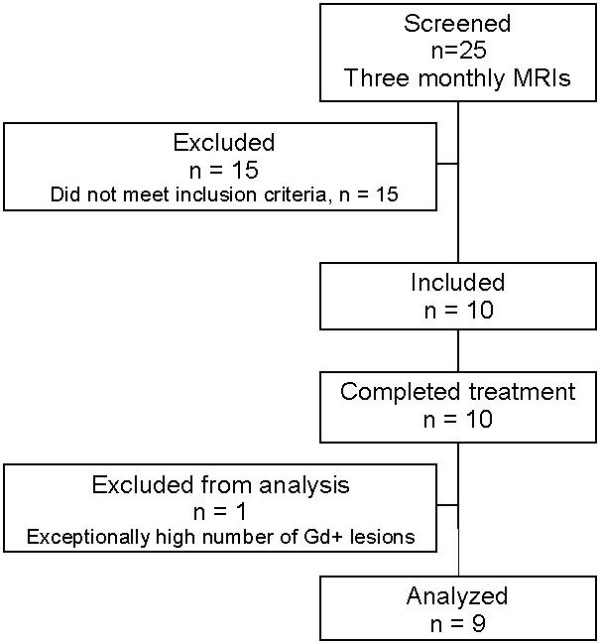
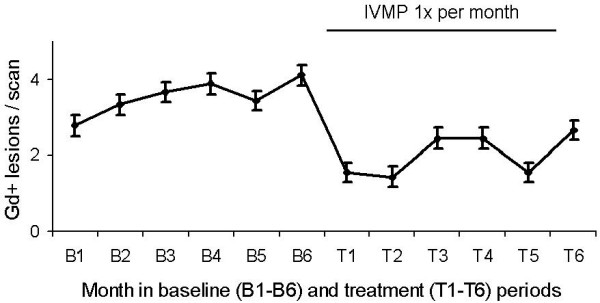
Methods: In an open, single-cross-over study, nine patients with relapsing-remitting MS (RR-MS) underwent cranial Gd-MRI once monthly for twelve months. From month six on, they received a single i.v.-infusion of 500 mg methylprednisolone (and oral tapering for three days) after the MRI. Primary outcome measure was the mean number of Gd+ lesions during treatment vs. baseline periods; T2 lesion volume and monthly plasma concentrations of cortisol, ACTH and prolactin were secondary outcome measures. Safety was assessed clinically, by routine laboratory and bone mineral density measurements. Soluble immune parameters (sTNF-RI, sTNF-RII, IL1-ra and sVCAM-1) and neuroendocrine tests (ACTH test, combined dexamethasone/CRH test) were additionally analyzed.
Results: Comparing treatment to baseline periods, the number of Gd+ lesions/scan was reduced in eight of the nine patients, by a median of 43.8% (p = 0.013, Wilcoxon). In comparison, a pooled dataset of 83 untreated RR-MS patients from several studies, selected by the same clinical and MRI criteria, showed a non-significant decrease by a median of 14% (p = 0.32). T2 lesion volume decreased by 21% during treatment (p = 0.001). Monthly plasma prolactin showed a parallel decline (p = 0.027), with significant cross-correlation with the number of Gd+ lesions. Other hormones and immune system variables were unchanged, as were ACTH test and dexamethasone-CRH test. Treatment was well tolerated; routine laboratory and bone mineral density were unchanged.
Conclusion: Monthly IV-MP reduces inflammatory activity and T2 lesion volume in RR-MS.
Figures
References
-
- Thompson AJ, Kennard C, Swash M, Summers B, Yuill GM, Shepherd DI, Roche S, Perkin GD, Loizou LA, Ferner R, Hughes RAC, Thompson M, Hand J. Relative efficacy of intravenous methylprednisolone and ACTH in the treatment of acute relapse in MS. Neurology. 1989;39:969–971. - PubMed
-
- Optic Neuritis Study Group The 5-year risk of MS after optic neuritis. Experience of the optic neuritis treatment trial. Neurology. 1997;49:1404–1413. - PubMed
-
- Beck RW, Trobe JD, Moke PS, Gal RL, Xing D, Bhatti MT, Brodsky MC, Buckley EG, Chrousos GA, Corbett J, Eggenberger E, Goodwin JA, Katz B, Kaufman DI, Keltner JL, Kupersmith MJ, Miller NR, Nazarian S, Orengo-Nania S, Savino PJ, Shults WT, Smith CH, Wall M. High- and low-risk profiles for the development of multiple sclerosis within 10 years after optic neuritis: experience of the optic neuritis treatment trial. Arch Ophthalmol. 2003;121:944–949. doi: 10.1001/archopht.121.7.944. - DOI - PubMed
-
- Kaufman DI, Trobe JD, Eggenberger ER, Whitaker JN. Practice parameter: The role of corticosteroids in the management of acute monosymptomatic optic neuritis: Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2000;54:2039–2044. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
