

Biomechanics and wound healing in the cornea
- PMID: 16720023
- PMCID: PMC2691611
- DOI: 10.1016/j.exer.2006.03.015
Biomechanics and wound healing in the cornea
Abstract
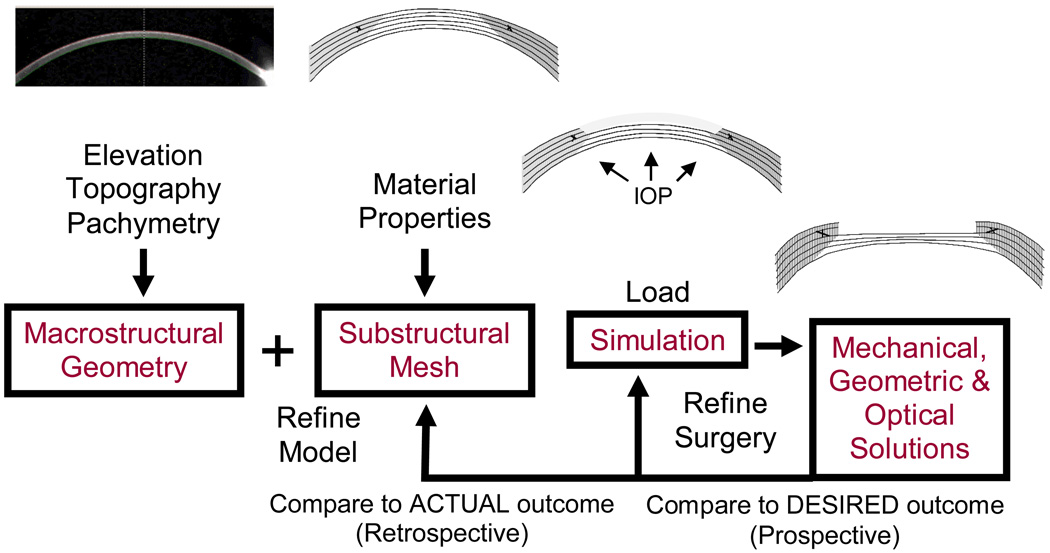
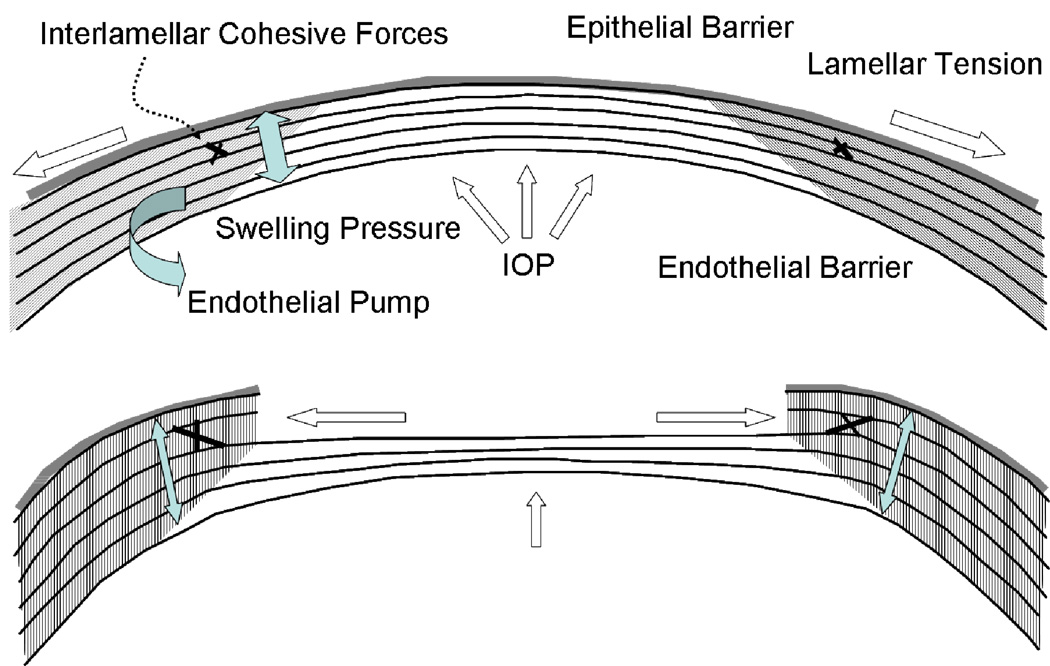
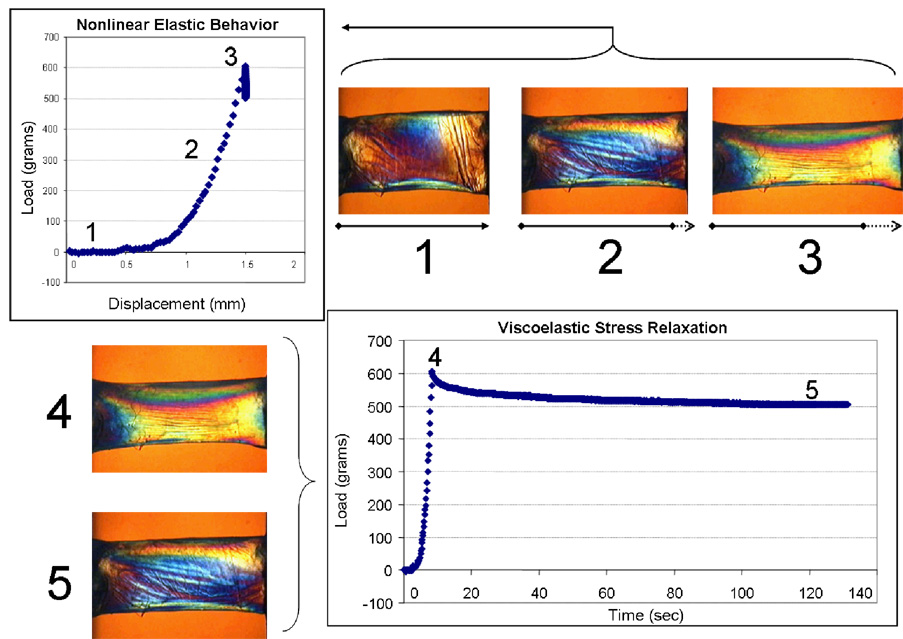
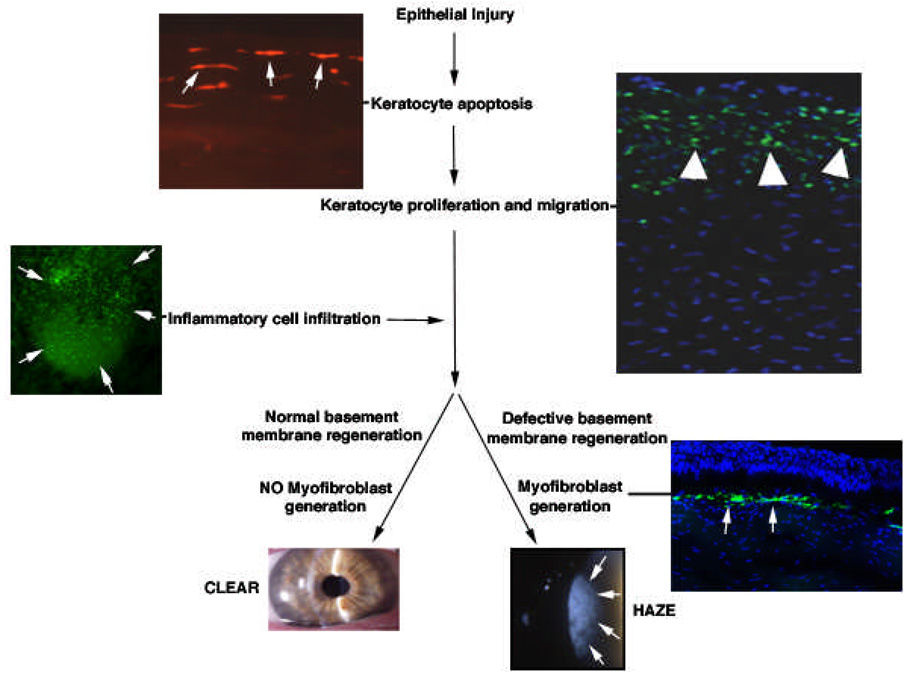
The biomechanical and wound healing properties of the cornea undermine the predictability and stability of refractive surgery and contribute to discrepancies between attempted and achieved visual outcomes after LASIK, surface ablation and other keratorefractive procedures. Furthermore, patients predisposed to biomechanical failure or abnormal wound healing can experience serious complications such as keratectasia or clinically significant corneal haze, and more effective means for the identification of such patients prior to surgery are needed. In this review, we describe the cornea as a complex structural composite material with pronounced anisotropy and heterogeneity, summarize current understanding of major biomechanical and reparative pathways that contribute to the corneal response to laser vision correction, and review the role of these processes in ectasia, intraocular pressure measurement artifact, diffuse lamellar keratitis (DLK) and corneal haze. The current understanding of differences in the corneal response after photorefractive keratectomy (PRK), LASIK and femtosecond-assisted LASIK are reviewed. Surgical and disease models that integrate corneal geometric data, substructural anatomy, elastic and viscoelastic material properties and wound healing behavior have the potential to improve clinical outcomes and minimize complications but depend on the identification of preoperative predictors of biomechanical and wound healing responses in individual patients.
Figures
Similar articles
-
Biomechanical and wound healing characteristics of corneas after excimer laser keratorefractive surgery: is there a difference between advanced surface ablation and sub-Bowman's keratomileusis?J Refract Surg. 2008 Jan;24(1):S90-6. doi: 10.3928/1081597X-20080101-16. J Refract Surg. 2008. PMID: 18269157
-
Corneal wound healing relevance to wavefront guided laser treatments.Ophthalmol Clin North Am. 2004 Jun;17(2):225-31, vii. doi: 10.1016/j.ohc.2004.03.002. Ophthalmol Clin North Am. 2004. PMID: 15207564 Review.
-
[Comparison of corneal wound healing of photorefractive keratectomy and laser in situ keratomileusis in rabbits].Zhonghua Yan Ke Za Zhi. 2003 Mar;39(3):140-5. Zhonghua Yan Ke Za Zhi. 2003. PMID: 12880569 Chinese.
-
Wound healing after keratorefractive surgery: review of biological and optical considerations.Cornea. 2012 Nov;31 Suppl 1(0 1):S9-19. doi: 10.1097/ICO.0b013e31826ab0a7. Cornea. 2012. PMID: 23038040 Free PMC article. Review.
-
Growth factors in corneal wound healing following refractive surgery: A review.Acta Ophthalmol Scand. 2002 Jun;80(3):238-47. doi: 10.1034/j.1600-0420.2002.800303.x. Acta Ophthalmol Scand. 2002. PMID: 12059860 Review.
Cited by
-
Keratocyte mechanobiology.Exp Eye Res. 2020 Nov;200:108228. doi: 10.1016/j.exer.2020.108228. Epub 2020 Sep 10. Exp Eye Res. 2020. PMID: 32919993 Free PMC article. Review.
-
Disorganized collagen scaffold interferes with fibroblast mediated deposition of organized extracellular matrix in vitro.Biotechnol Bioeng. 2012 Oct;109(10):2683-98. doi: 10.1002/bit.24533. Epub 2012 May 4. Biotechnol Bioeng. 2012. PMID: 22528405 Free PMC article.
-
A structural model for the in vivo human cornea including collagen-swelling interaction.J R Soc Interface. 2015 Aug 6;12(109):20150241. doi: 10.1098/rsif.2015.0241. J R Soc Interface. 2015. PMID: 26156299 Free PMC article.
-
Value of corneal epithelial and Bowman's layer vertical thickness profiles generated by UHR-OCT for sub-clinical keratoconus diagnosis.Sci Rep. 2016 Aug 11;6:31550. doi: 10.1038/srep31550. Sci Rep. 2016. PMID: 27511620 Free PMC article. Clinical Trial.
-
Simulation of Air Puff Tonometry Test Using Arbitrary Lagrangian-Eulerian (ALE) Deforming Mesh for Corneal Material Characterisation.Int J Environ Res Public Health. 2019 Dec 19;17(1):54. doi: 10.3390/ijerph17010054. Int J Environ Res Public Health. 2019. PMID: 31861736 Free PMC article.
References
-
- Andreassen TT, Simonsen AH, Oxlund H. Biomechanical properties of keratoconus and normal corneas. Exp Eye Res. 1980;31:435–441. - PubMed
-
- Bhawan J, Majno G. The myofibroblast. Possible derivation from macrophages in xanthogranuloma. Am J Dermatopathol. 1989;11:255–258. - PubMed
-
- Binder PS. Flap dimensions created with the IntraLase FS laser. J Cataract Refract Surg. 2004;30:26–32. - PubMed
-
- Bissen-Miyajima H, Nakamura K, Kaido M, Shimmura S, Tsubota K. Role of the endothelial pump in flap adhesion after laser in situ keratomileusis. J Cataract Refract Surg. 2004;30:1989–1992. - PubMed
-
- Brandt JD, Beiser JA, Kass MA, Gordon MO. Central corneal thickness in the Ocular Hypertension Treatment Study (OHTS) Ophthalmology. 2001;108:1779–1788. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
