

Survival following adjuvant PCV or temozolomide for anaplastic astrocytoma
- PMID: 16723632
- PMCID: PMC1871946
- DOI: 10.1215/15228517-2006-005
Survival following adjuvant PCV or temozolomide for anaplastic astrocytoma
Abstract
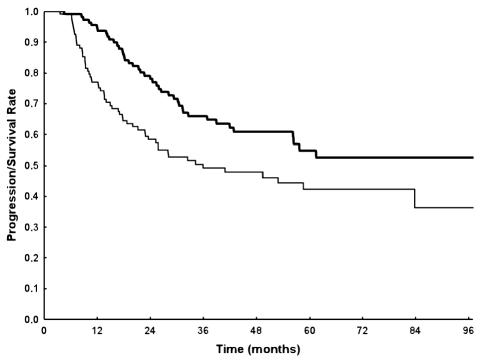
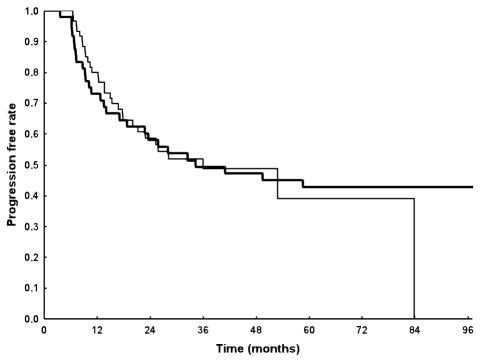
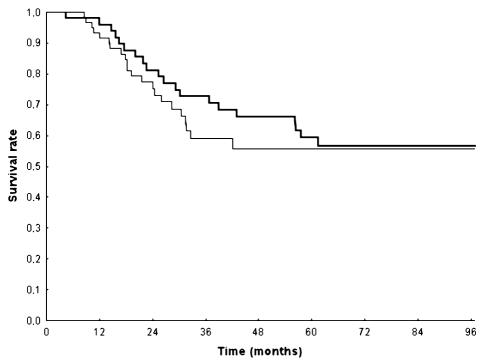
We compared survival in patients with anaplastic astrocytoma (AA) treated with adjuvant procarbazine, lomustine, and vincristine (PCV) with survival in patients treated with temozolomide. A retrospective analysis was made of patients with newly diagnosed AA treated with adjuvant postradiotherapy chemotherapy. Outcome analysis included progression-free survival and overall survival. The following prognostic factors were taken into account: patient age, extent of resection, performance status, presence of contrast enhancement in presurgical imaging, and type of adjuvant treatment. Among 109 AA patients, 49 were treated with PCV and 60 with temozolomide. The treatment groups were well matched for pretreatment characteristics, except for the presence of contrast enhancement. Age, extent of surgery, performance status, and presence of contrast enhancement were statistically significant prognostic factors according to the Cox model analysis of survival. Type of adjuvant chemotherapy was not a significant factor, either for progression-free survival or for overall survival. Hematological toxicity, nonhematological toxicity grades 3-4, and premature discontinuation due to toxicity were observed in 9%, 3% to 5%, and 37%, respectively, of cases in the PCV group versus 4% to 5%, 0, and 0, respectively, in the temozolomide group. Although the present study was not randomized, it was well designed, and it reports on two homogeneous and consecutive series of patients, for whom histology was verified to obtain survival data only for patients with AA following the recent WHO 2000 classification. Even if no survival advantage has been demonstrated for temozolomide versus PCV, we conclude that temozolomide should be preferred because of its greater tolerability.
Figures
References
-
- Buckner JC. Factors influencing survival in high-grade gliomas. Semin Oncol. 2003;30:10–14. - PubMed
-
- CBTRUS, Central Brain Tumor Registry of the United States (2004) Primary Brain Tumors in the United States: Statistical Report, 1997–2001 Available at http://www.cbtrus.org/2004-2005/2004-2005.html
-
- Cohen ZR, Suki D, Shi W, Weinberg JS, DeMonte F, McCutcheon IE, Hassenbusch SJ, Gokaslan ZL, Rhines LD, Sawaya R, Lang FF. Surgical resection of anaplastic astrocytoma: Prognostic factors and outcome. Neuro-Oncology. 2002;4:367. (abstract 216)
-
- Cox D. Regression models and life-tables. J R Stat Soc B. 1972;34:187–220.
-
- Curran WJ, Jr, Scott CB, Horton J, Nelson JS, Weinstein AS, Fischbach AJ, Chang CH, Rotman M, Asbell SO, Krisch RE, Nelson DF. Recursive partitioning analysis of prognostic factors in three Radiation Therapy Oncology Group malignant glioma trials. J Natl Cancer Inst. 1993;85:704–710. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
