

The fraction of ischaemic heart disease and stroke attributable to smoking in the WHO Western Pacific and South-East Asian regions
- PMID: 16728748
- PMCID: PMC2564655
- DOI: 10.1136/tc.2005.013284
The fraction of ischaemic heart disease and stroke attributable to smoking in the WHO Western Pacific and South-East Asian regions
Abstract
Background: Tobacco will soon be the biggest cause of death worldwide, with the greatest burden being borne by low and middle-income countries where 8/10 smokers now live.
Objective: This study aimed to quantify the direct burden of smoking for cardiovascular diseases (CVD) by calculating the population attributable fractions (PAF) for fatal ischaemic heart disease (IHD) and stroke (haemorrhagic and ischaemic) for all 38 countries in the World Health Organization Western Pacific and South East Asian regions.
Design and subjects: Sex-specific prevalence of smoking was obtained from existing data. Estimates of the hazard ratio (HR) for IHD and stroke with smoking as an independent risk factor were obtained from the approximately 600,000 adult subjects in the Asia Pacific Cohort Studies Collaboration (APCSC). HR estimates and prevalence were then used to calculate sex-specific PAF for IHD and stroke by country.
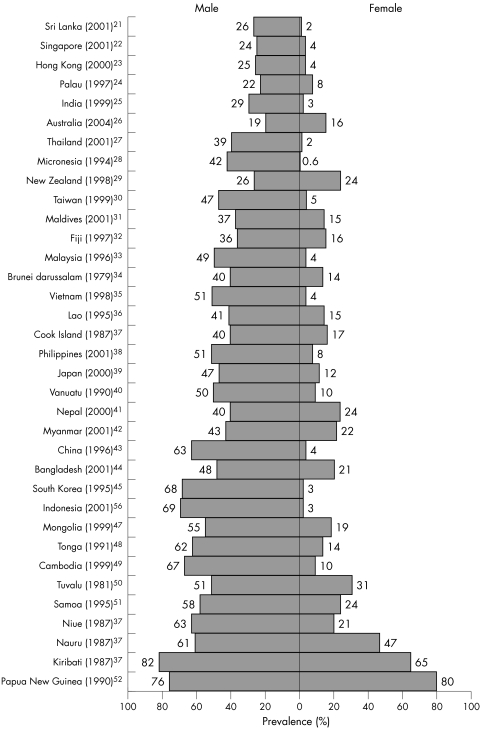
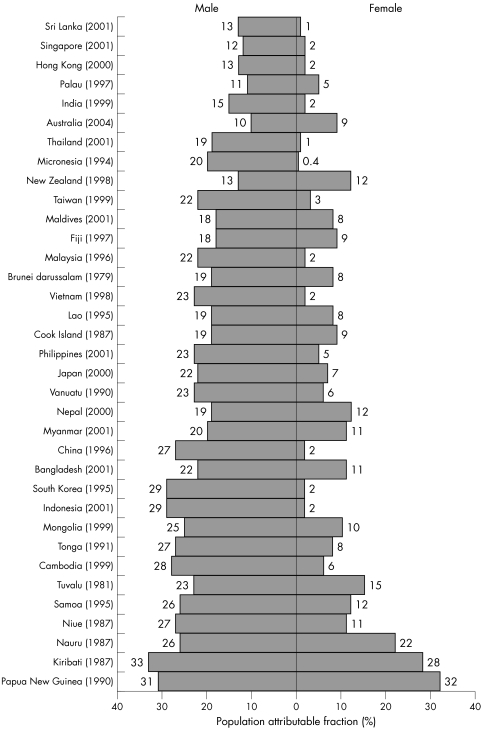
Results: The prevalence of smoking in the 33 countries, for which relevant data could be obtained, ranged from 28-82% in males and from 1-65% in females. The fraction of IHD attributable to smoking ranged from 13-33% in males and from <1-28% in females. The percentage of haemorrhagic stroke attributable to smoking ranged from 4-12% in males and from <1-9% in females. Corresponding figures for ischaemic stroke were 11-27% in males and <1-22% in females.
Conclusions: Up to 30% of some cardiovascular fatalities can be attributed to smoking. This is likely an underestimate of the current burden of smoking on CVD, given that the smoking epidemic has developed further since many of the studies were conducted.
Conflict of interest statement
The authors declare no known competing interests.


References
-
- Jha P, Chaloupka F J, Brown P.Tobacco control in developing countries: curbing the epidemic. (Chapter 1: Overview). World Bank: Economics of Tobacco Control, 2000. http://www1.worldbank.org/tobacco/tcdc.asp (Accessed March 31, 2005)
-
- Leeder S, Raymond S, Greenberg H.et alA race against time: the challenge of cardiovascular disease in developing economies. New York: Columbia University, 2004
-
- Gajalakshmi C K, Jha P, Ranson K.et alTobacco control in developing countries: curbing the epidemic. (Chapter 2: Global patterns of smoking and smoking attributable mortality). World Bank: Economics of Tobacco Control, 2000. http://www1.worldbank.org/tobacco/tcdc.asp (Accessed March 31, 2005)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical