

Rational prescribing in primary care (RaPP): a cluster randomized trial of a tailored intervention
- PMID: 16737346
- PMCID: PMC1472695
- DOI: 10.1371/journal.pmed.0030134
Rational prescribing in primary care (RaPP): a cluster randomized trial of a tailored intervention
Abstract
Background: A gap exists between evidence and practice regarding the management of cardiovascular risk factors. This gap could be narrowed if systematically developed clinical practice guidelines were effectively implemented in clinical practice. We evaluated the effects of a tailored intervention to support the implementation of systematically developed guidelines for the use of antihypertensive and cholesterol-lowering drugs for the primary prevention of cardiovascular disease.
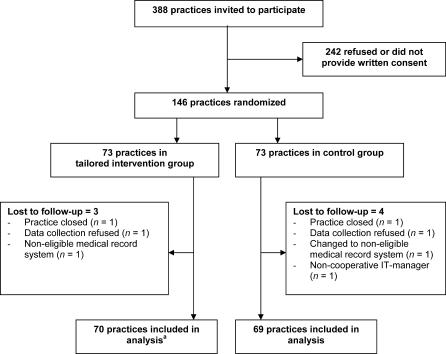
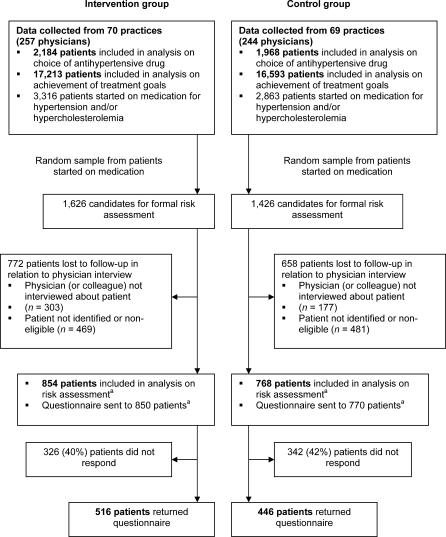
Methods and findings: We conducted a cluster-randomized trial comparing a tailored intervention to passive dissemination of guidelines in 146 general practices in two geographical areas in Norway. Each practice was randomized to either the tailored intervention (70 practices; 257 physicians) or control group (69 practices; 244 physicians). Patients started on medication for hypertension or hypercholesterolemia during the study period and all patients already on treatment that consulted their physician during the trial were included. A multifaceted intervention was tailored to address identified barriers to change. Key components were an educational outreach visit with audit and feedback, and computerized reminders linked to the medical record system. Pharmacists conducted the visits. Outcomes were measured for all eligible patients seen in the participating practices during 1 y before and after the intervention. The main outcomes were the proportions of (1) first-time prescriptions for hypertension where thiazides were prescribed, (2) patients assessed for cardiovascular risk before prescribing antihypertensive or cholesterol-lowering drugs, and (3) patients treated for hypertension or hypercholesterolemia for 3 mo or more who had achieved recommended treatment goals. The intervention led to an increase in adherence to guideline recommendations on choice of antihypertensive drug. Thiazides were prescribed to 17% of patients in the intervention group versus 11% in the control group (relative risk 1.94; 95% confidence interval 1.49-2.49, adjusted for baseline differences and clustering effect). Little or no differences were found for risk assessment prior to prescribing and for achievement of treatment goals.
Conclusions: Our tailored intervention had a significant impact on prescribing of antihypertensive drugs, but was ineffective in improving the quality of other aspects of managing hypertension and hypercholesterolemia in primary care.
Conflict of interest statement
Figures
Comment in
-
Improving prescribing practices in primary care. A randomised trial and economic analysis of a multicomponent intervention showed small, but important, gains.PLoS Med. 2006 Jun;3(6):e229. doi: 10.1371/journal.pmed.0030229. PLoS Med. 2006. PMID: 16729845 Free PMC article.
-
What guidelines? Never saw them!PLoS Med. 2006 Sep;3(9):e413; author reply e414. doi: 10.1371/journal.pmed.0030413. PLoS Med. 2006. PMID: 17002513 Free PMC article. No abstract available.
References
-
- Collins R, Peto R, MacMahon S, Hebert P, Fiebach NH, et al. Blood pressure, stroke, and coronary heart disease. Part 2, Short-term reductions in blood pressure: Overview of randomised drug trials in their epidemiological context. Lancet. 1990;335:827–838. - PubMed
-
- LaRosa JC, He J, Vupputuri S. Effect of statins on risk of coronary disease: A meta-analysis of randomized controlled trials. JAMA. 1999;282:2340–2346. - PubMed
-
- Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess. 2004;8:1–72. - PubMed
-
- Fretheim A, Bjørndal A, Oxman AD, Dyrdal A, Golding M, et al. Hvilke kolesterolsenkende legemidler bør brukes for primærforebygging av hjerte- og karsykdommer? Tidsskr Nor Laegeforen. 2002;122:2287–2288. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
