

Rational prescribing in primary care (RaPP): economic evaluation of an intervention to improve professional practice
- PMID: 16737349
- PMCID: PMC1472698
- DOI: 10.1371/journal.pmed.0030216
Rational prescribing in primary care (RaPP): economic evaluation of an intervention to improve professional practice
Abstract
Background: Interventions designed to narrow the gap between research findings and clinical practice may be effective, but also costly. Economic evaluations are necessary to judge whether such interventions are worth the effort. We have evaluated the economic effects of a tailored intervention to support the implementation of guidelines for the use of antihypertensive and cholesterol-lowering drugs. The tailored intervention was evaluated in a randomized trial, and was shown to significantly increase the use of thiazides for patients started on antihypertensive medication, but had little or no impact on other outcomes. The increased use of thiazides was not expected to have an impact on health outcomes.
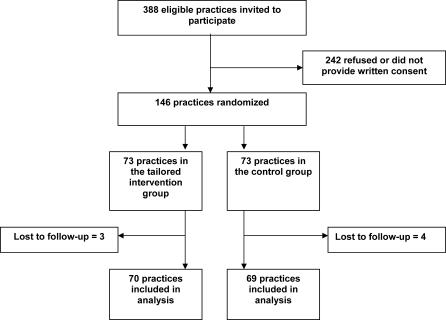
Methods and findings: We performed cost-minimization and cost-effectiveness analyses on data from a randomized trial involving 146 general practices from two geographical areas in Norway. Each practice was randomized to either the tailored intervention (70 practices; 257 physicians) or control group (69 practices; 244 physicians). Only patients that were being started on antihypertensive medication were included in the analyses. A multifaceted intervention was tailored to address identified barriers to change. Key components were an educational outreach visit with audit and feedback, and computerized reminders. Pharmacists conducted the visits. A cost-minimization framework was adopted, where the costs of intervention were set against the reduced treatment costs (principally due to increased use of thiazides rather than more expensive medication). The cost-effectiveness of the intervention was estimated as the cost per additional patient being started on thiazides. The net annual cost (cost minimization) in our study population was 53,395 US dollars, corresponding to 763 US dollars per practice. The cost per additional patient started on thiazides (cost-effectiveness) was 454 US dollars. The net annual savings in a national program was modeled to be 761,998 US dollars, or 540 US dollars per practice after 2 y. In this scenario the savings exceeded the costs in all but two of the sensitivity analyses we conducted, and the cost-effectiveness was estimated to be 183 US dollars.
Conclusions: We found a significant shift in prescribing of antihypertensive drugs towards the use of thiazides in our trial. A major reason to promote the use of thiazides is their lower price compared to other drugs. The cost of the intervention was more than twice the savings within the time frame of our study. However, we predict modest savings over a 2-y period.
Conflict of interest statement
Figures
Comment in
-
Improving prescribing practices in primary care. A randomised trial and economic analysis of a multicomponent intervention showed small, but important, gains.PLoS Med. 2006 Jun;3(6):e229. doi: 10.1371/journal.pmed.0030229. PLoS Med. 2006. PMID: 16729845 Free PMC article.
References
-
- Grimshaw JM, Shirran L, Thomas R, Mowatt G, Fraser C, et al. Changing provider behavior: An overview of systematic reviews of interventions. Med Care. 2001;39:II2–II45. - PubMed
-
- Grimshaw JM, Thomas RE, MacLennan G, Fraser C, Ramsay CR, et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol Assess. 2004;8:1–72. - PubMed
-
- Turnbull F Blood Pressure Lowering Treatment Trialists' Collaboration. Effects of different blood-pressure-lowering regimens on major cardiovascular events: Results of prospectively-designed overviews of randomised trials. Lancet. 2003;362:1527–1535. - PubMed
-
- Psaty BM, Lumley T, Furberg CD, Schellenbaum G, Pahor M, et al. Health outcomes associated with various antihypertensive therapies used as first-line agents: A network meta-analysis. JAMA. 2003;289:2534–2544. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
