

Body-mass index and symptoms of gastroesophageal reflux in women
- PMID: 16738270
- PMCID: PMC2782772
- DOI: 10.1056/NEJMoa054391
Body-mass index and symptoms of gastroesophageal reflux in women
Abstract
Background: Overweight and obese persons are at increased risk for gastroesophageal reflux disease. An association between body-mass index (BMI)--the weight in kilograms divided by the square of the height in meters - and symptoms of gastroesophageal reflux disease in persons of normal weight has not been demonstrated.
Methods: In 2000, we used a supplemental questionnaire to determine the frequency, severity, and duration of symptoms of gastroesophageal reflux disease among randomly selected participants in the Nurses' Health Study. After categorizing women according to BMI as measured in 1998, we used logistic-regression models to study the association between BMI and symptoms of gastroesophageal reflux disease.
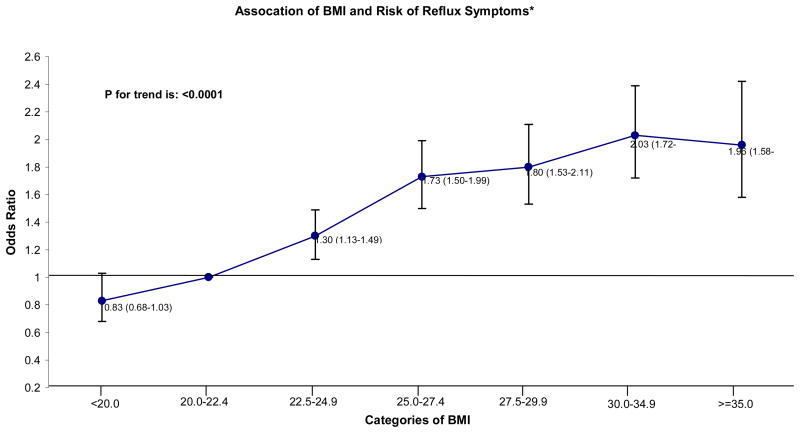
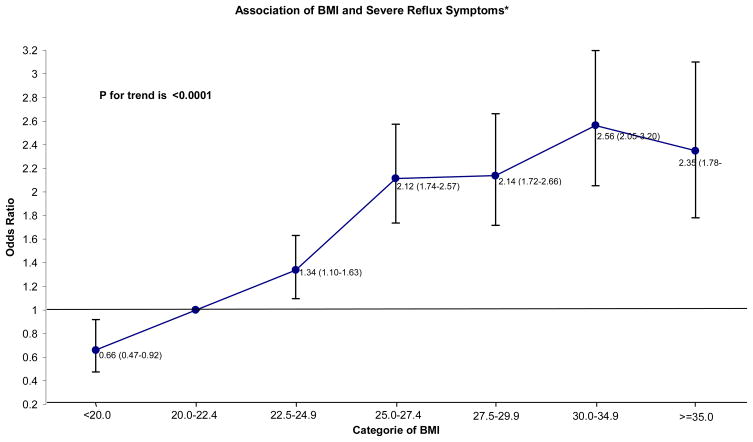
Results: Of 10,545 women who completed the questionnaire (response rate, 86 percent), 2310 (22 percent) reported having symptoms at least once a week, and 3419 (55 percent of those who had any symptoms) described their symptoms as moderate in severity. We observed a dose-dependent relationship between increasing BMI and frequent reflux symptoms (multivariate P for trend <0.001). As compared with women who had a BMI of 20.0 to 22.4, the multivariate odds ratios for frequent symptoms were 0.67 (95 percent confidence interval, 0.48 to 0.93) for a BMI of less than 20.0, 1.38 (95 percent confidence interval, 1.13 to 1.67) for a BMI of 22.5 to 24.9, 2.20 (95 percent confidence interval, 1.81 to 2.66) for a BMI of 25.0 to 27.4, 2.43 (95 percent confidence interval, 1.96 to 3.01) for a BMI of 27.5 to 29.9, 2.92 (95 percent confidence interval, 2.35 to 3.62) for a BMI of 30.0 to 34.9, and 2.93 (95 percent confidence interval, 2.24 to 3.85) for a BMI of 35.0 or more. Even in women with a normal baseline BMI, an increase in BMI of more than 3.5, as compared with no weight changes, was associated with an increased risk of frequent symptoms of reflux (odds ratio, 2.80; 95 percent confidence interval, 1.63 to 4.82).
Conclusions: BMI is associated with symptoms of gastroesophageal reflux disease in both normal-weight and overweight women. Even moderate weight gain among persons of normal weight may cause or exacerbate symptoms of reflux.
Copyright 2006 Massachusetts Medical Society.
Figures
Comment in
-
BMI and gastroesophageal reflux in women.N Engl J Med. 2006 Aug 24;355(8):848; author reply 849-50. doi: 10.1056/NEJMc061773. N Engl J Med. 2006. PMID: 16929003 No abstract available.
-
BMI and gastroesophageal reflux in women.N Engl J Med. 2006 Aug 24;355(8):848-9; author reply 849-50. N Engl J Med. 2006. PMID: 16937552 No abstract available.
-
BMI and gastroesophageal reflux in women.N Engl J Med. 2006 Aug 24;355(8):848; author reply 849-50. N Engl J Med. 2006. PMID: 16937553 No abstract available.
References
-
- Klauser A, Schindlbeck N, Muller-Lissner SA. Symptoms in gastro-oesophageal reflux disease. Lancet. 1990;335:205–208. - PubMed
-
- Locke GR, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448–1456. - PubMed
-
- El-Serag H, Petersen N, Carter J, et al. Gastroesophageal reflux among different racial groups in the United States. Gastroenterology. 2004;126:1692–1699. - PubMed
-
- Sandler R, Everhart J, Donowitz M, et al. The burden of selected digestive diseases in the United States. Gastroenterology. 2002;122:1500–1511. - PubMed
-
- Henke C, Levin T, Henning J, Potter L. Work loss costs due to peptic ulcer disease and gastroesophageal reflux disease in a health maintenance organization. Am J Gastroenterol. 2000;95:788–792. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials