

Orthopedic complications of overweight in children and adolescents
- PMID: 16740861
- PMCID: PMC1863007
- DOI: 10.1542/peds.2005-1832
Orthopedic complications of overweight in children and adolescents
Abstract
Objective: Few studies have quantified the prevalence of weight-related orthopedic conditions in otherwise healthy overweight children. The goal of the present investigation was to describe the musculoskeletal consequences of pediatric overweight in a large pediatric cohort of children that included severely overweight children.
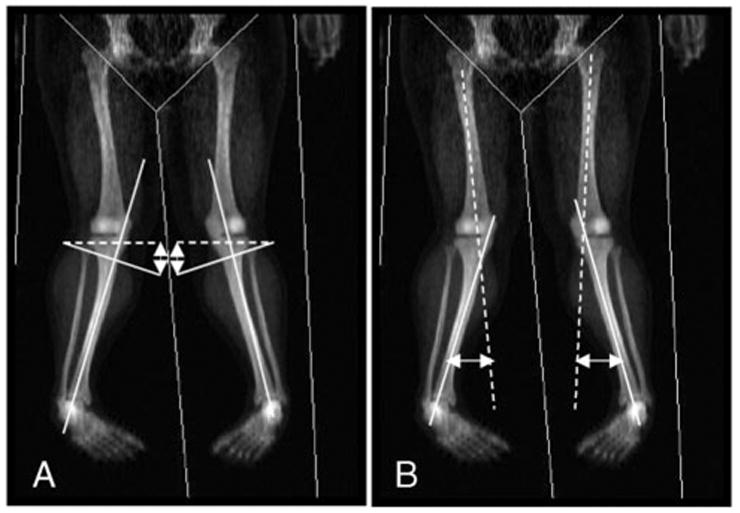
Methods: Medical charts from 227 overweight and 128 nonoverweight children and adolescents who were enrolled in pediatric clinical studies at the National Institutes of Health from 1996 to 2004 were reviewed to record pertinent orthopedic medical history and musculoskeletal complaints. Questionnaire data from 183 enrollees (146 overweight) documented difficulties with mobility. In 250, lower extremity alignment was determined by bilateral metaphyseal-diaphyseal and anatomic tibiofemoral angle measurements made from whole-body dual-energy x-ray absorptiometry scans.
Results: Compared with nonoverweight children, overweight children reported a greater prevalence of fractures and musculoskeletal discomfort. The most common self-reported joint complaint among those who were questioned directly was knee pain (21.4% overweight vs 16.7% nonoverweight). Overweight children reported greater impairment in mobility than did nonoverweight children (mobility score: 17.0 +/- 6.8 vs 11.6 +/- 2.8). Both metaphyseal-diaphyseal and anatomic tibiofemoral angle measurements showed greater malalignment in overweight compared with nonoverweight children.
Conclusions: Reported fractures, musculoskeletal discomfort, impaired mobility, and lower extremity malalignment are more prevalent in overweight than nonoverweight children and adolescents. Because they affect the likelihood that children will engage in physical activity, orthopedic difficulties may be part of the cycle that perpetuates the accumulation of excess weight in children.
Figures


References
-
- Hedley AA, Ogden CL, Johnson CL, Carroll MD, Curtin LR, Flegal KM. Prevalence of overweight and obesity among US children, adolescents, and adults, 1999–2002. JAMA. 2004;291:2847–2850. - PubMed
-
- Ogden CL, Flegal KM, Carroll MD, Johnson CL. Prevalence and trends in overweight among US children and adolescents, 1999–2000. JAMA. 2002;288:1728–1732. - PubMed
-
- Must A, Strauss RS. Risks and consequences of childhood and adolescent obesity. Int J Obes Relat Metab Disord. 1999;23(suppl 2):S2–S11. - PubMed
-
- Dougados M, Gueguen A, Nguyen M, et al. Longitudinal radiologic evaluation of osteoarthritis of the knee. J Rheumatol. 1992;19:378–384. - PubMed
-
- Cohen NP, Foster RJ, Mow VC. Composition and dynamics of articular cartilage: structure, function, and maintaining healthy state. J Orthop Sports Phys Ther. 1998;28:203–215. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
