

Treatment of anisometropic amblyopia in children with refractive correction
- PMID: 16751032
- PMCID: PMC1790727
- DOI: 10.1016/j.ophtha.2006.01.068
Treatment of anisometropic amblyopia in children with refractive correction
Abstract
Objective: To evaluate the effectiveness of refractive correction alone for the treatment of untreated anisometropic amblyopia in children 3 to <7 years old.
Design: Prospective, multicenter, noncomparative intervention.
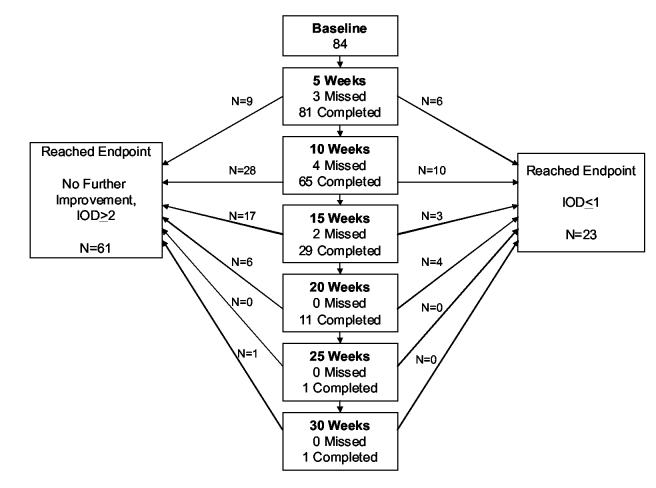
Participants: Eighty-four children 3 to <7 years old with untreated anisometropic amblyopia ranging from 20/40 to 20/250.
Methods: Optimal refractive correction was provided, and visual acuity (VA) was measured with the new spectacle correction at baseline and at 5-week intervals until VA stabilized or amblyopia resolved.
Main outcome measures: Maximum improvement in best-corrected VA in the amblyopic eye and proportion of children whose amblyopia resolved (interocular difference of < or =1 line) with refractive correction alone.
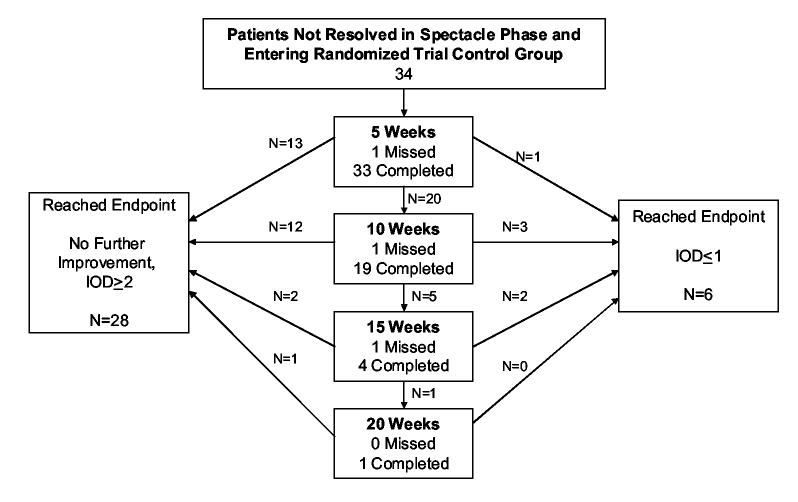
Results: Amblyopia improved with optical correction by > or =2 lines in 77% of the patients and resolved in 27%. Improvement took up to 30 weeks for stabilization criteria to be met. After stabilization, additional improvement occurred with spectacles alone in 21 of 34 patients observed in a control group of a subsequent randomized trial, with amblyopia resolving in 6. Treatment outcome was not related to age, but was related to better baseline VA and lesser amounts of anisometropia.
Conclusion: Refractive correction alone improves VA in many cases and results in resolution of amblyopia in at least one third of 3- to <7-year-old children with untreated anisometropic amblyopia. Although most cases of resolution occur with moderate (20/40-20/100) amblyopia, the average 3-line improvement in VA resulting from treatment with spectacles may lessen the burden of subsequent amblyopia therapy for those with denser levels of amblyopia.
Figures
Comment in
-
Amblyopia can be treated without occlusion or atropine.Ophthalmology. 2006 Jun;113(6):893. doi: 10.1016/j.ophtha.2006.04.010. Ophthalmology. 2006. PMID: 16751031 No abstract available.
References
-
- Pediatric Eye Disease Investigator Group The clinical profile of moderate amblyopia in children younger than 7 years. Arch Ophthalmol. 2002;120:281–7. - PubMed
-
- Kivlin JD, Flynn JT. Therapy of anisometropic amblyopia. J Pediatr Ophthalmol Strabismus. 1981;18:47–56. - PubMed
-
- Clarke WN, Noel LP. Prognostic indicators for avoiding occlusion therapy in anisometropic amblyopia. American Orthoptic Journal. 1990;40:57–63.
-
- Krumholtz I, FitzGerald D. Efficacy of treatment modalities in refractive amblyopia. J Am Optom Assoc. 1999;70:399–404. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
