

Inequalities in hospital admission rates for unintentional poisoning in young children
- PMID: 16751446
- PMCID: PMC2563534
- DOI: 10.1136/ip.2005.011254
Inequalities in hospital admission rates for unintentional poisoning in young children
Abstract
Objective: To determine the relationship between deprivation and hospital admission rates for unintentional poisoning, by poisoning agent in children aged 0-4 years.
Design: Cross sectional study of routinely collected hospital admissions data.
Setting: East Midlands, UK.
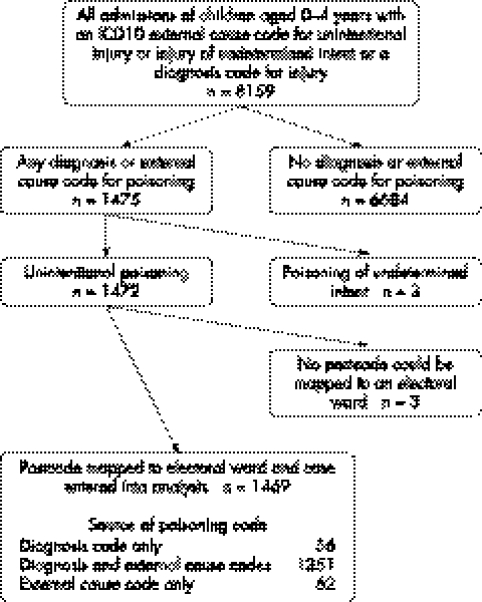
Participants: 1469 admissions due to unintentional poisoning over two years.
Main outcome measure: Hospital admission rates for unintentional poisoning. Incidence rate ratios (IRRs) comparing hospital admission rates for poisoning in the most and least deprived electoral wards.
Results: Children in the most deprived wards had admission rates for medicinal poisoning that were 2-3 times higher than those in the least deprived wards (IRR 2.49, 95% CI 1.87 to 3.30). Admission rates for non-medicinal poisoning were about twice as high in the most compared to the least deprived wards (IRR 1.77, 95% CI 1.19 to 2.64). Deprivation gradients were particularly steep for benzodiazepines (IRR 5.63, 95% CI 1.72 to 18.40), antidepressants (IRR 4.58, 95% CI 1.80 to 11.66), cough and cold remedies (IRR 3.93, 95% CI 1.67 to 9.24), and organic solvents (IRR 3.69, 95% CI 1.83 to 7.44).
Conclusions: There are steep deprivation gradients for admissions to hospital for childhood poisoning, with particularly steep gradients for some psychotropic medicines. Interventions to reduce these inequalities should be directed towards areas of greater deprivation.
Conflict of interest statement
Competing interests: none.
Similar articles
-
Hospital admissions for unintentional poisoning in preschool children in England; 2000-2011.Arch Dis Child. 2015 Feb;100(2):180-2. doi: 10.1136/archdischild-2013-305298. Epub 2014 Aug 28. Arch Dis Child. 2015. PMID: 25169824
-
Some epidemiological observations on medicinal and non-medicinal poisoning in preschool children.J Epidemiol Community Health. 1992 Jun;46(3):207-10. doi: 10.1136/jech.46.3.207. J Epidemiol Community Health. 1992. PMID: 1645072 Free PMC article.
-
Cross sectional survey of socioeconomic variations in severity and mechanism of childhood injuries in Trent 1992-7.BMJ. 2002 May 11;324(7346):1132. doi: 10.1136/bmj.324.7346.1132. BMJ. 2002. PMID: 12003886 Free PMC article.
-
Inequalities in hip fracture incidence are greatest in the North of England: regional analysis of the effects of social deprivation on hip fracture incidence across England.Public Health. 2018 Sep;162:25-31. doi: 10.1016/j.puhe.2018.05.002. Epub 2018 Jun 23. Public Health. 2018. PMID: 29945041
-
First aid interventions by laypeople for acute oral poisoning.Cochrane Database Syst Rev. 2018 Dec 19;12(12):CD013230. doi: 10.1002/14651858.CD013230. Cochrane Database Syst Rev. 2018. PMID: 30565220 Free PMC article.
Cited by
-
Socio-economic inequities in children's injury rates: has the gradient changed over time?Can J Public Health. 2010 Nov-Dec;101 Suppl 3(Suppl 3):S28-31. doi: 10.1007/BF03405575. Can J Public Health. 2010. PMID: 21416816 Free PMC article. English, French.
-
20 Years of Research on Socioeconomic Inequality and Children's-Unintentional Injuries Understanding the Cause-Specific Evidence at Hand.Int J Pediatr. 2010;2010:819687. doi: 10.1155/2010/819687. Epub 2010 Jul 25. Int J Pediatr. 2010. PMID: 20706660 Free PMC article.
-
Socio-demographic patterns in hospital admissions and accident and emergency attendances among young people using linkage to NHS Hospital Episode Statistics: results from the Avon Longitudinal Study of Parents and Children.BMC Health Serv Res. 2019 Feb 26;19(1):134. doi: 10.1186/s12913-019-3922-7. BMC Health Serv Res. 2019. PMID: 30808346 Free PMC article.
-
Independent risk factors for injury in pre-school children: three population-based nested case-control studies using routine primary care data.PLoS One. 2012;7(4):e35193. doi: 10.1371/journal.pone.0035193. Epub 2012 Apr 5. PLoS One. 2012. PMID: 22496906 Free PMC article.
-
Patterns and trends of medicinal poisoning substances: a population-based cohort study of injuries in 0-11 year old children from 1998-2018.Arch Public Health. 2024 Apr 16;82(1):50. doi: 10.1186/s13690-024-01268-7. Arch Public Health. 2024. PMID: 38627812 Free PMC article.
References
-
- Department of Trade and Industry 24th (Final) Report of the Home and Leisure Accident Surveillance System. London: Department of Trade and Industry, 2003
-
- Department of Health Hospital Episode Statistics 2002/3. London: Department of Health, 2004
-
- Office for National Statistics Mortality statistics: cause. Review of the Registrar General on deaths by cause, sex and age, in England and Wales, 2002. London: Office for National Statistics, 2003
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical