

Hypotonic versus isotonic saline in hospitalised children: a systematic review
- PMID: 16754657
- PMCID: PMC2066024
- DOI: 10.1136/adc.2005.088690
Hypotonic versus isotonic saline in hospitalised children: a systematic review
Abstract
Background: The traditional recommendations which suggest that hypotonic intravenous (i.v.) maintenance fluids are the solutions of choice in paediatric patients have not been rigorously tested in clinical trials, and may not be appropriate for all children.
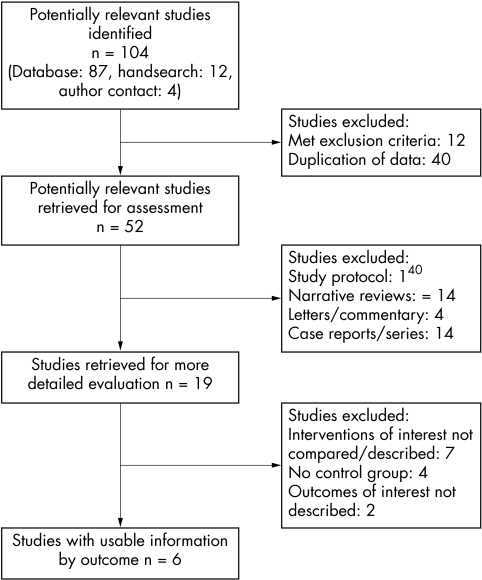
Aims: To systematically review the evidence from studies evaluating the safety of administering hypotonic versus isotonic i.v. maintenance fluids in hospitalised children.
Data sources: Medline (1966-2006), Embase (1980-2006), the Cochrane Library, abstract proceedings, personal files, and reference lists. Studies that compared hypotonic to isotonic maintenance solutions in children were selected. Case reports and studies in neonates or patients with a pre-existing history of hyponatraemia were excluded.
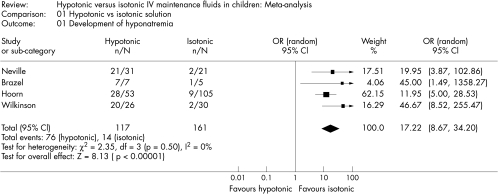
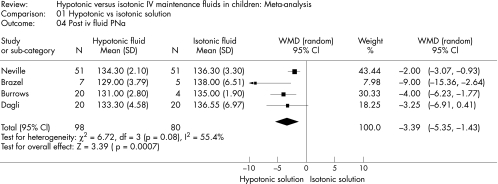
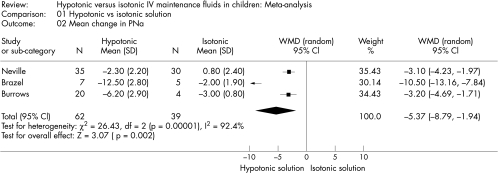
Results: Six studies met the selection criteria. A meta-analysis combining these studies showed that hypotonic solutions significantly increased the risk of developing acute hyponatraemia (OR 17.22; 95% CI 8.67 to 34.2), and resulted in greater patient morbidity.
Conclusions: The current practice of prescribing i.v. maintenance fluids in children is based on limited clinical experimental evidence from poorly and differently designed studies, where bias could possibly raise doubt about the results. They do not provide evidence for optimal fluid and electrolyte homoeostasis in hospitalised children. This systematic review indicates potential harm with hypotonic solutions in children, which can be anticipated and avoided with isotonic solutions. No single fluid rate or composition is ideal for all children. However, isotonic or near-isotonic solutions may be more physiological, and therefore a safer choice in the acute phase of illness and perioperative period.
Conflict of interest statement
Competing interests: none declared
Comment in
-
Review: hypotonic solutions increase acute hyponatraemia in children receiving standard intravenous maintenance therapy.Evid Based Nurs. 2007 Apr;10(2):59. doi: 10.1136/ebn.10.2.59. Evid Based Nurs. 2007. PMID: 17384111 No abstract available.
References
-
- Holliday M A, Segar M E. The maintenance need for water in parenteral fluid therapy. Pediatrics 195719823–832. - PubMed
-
- Wallace W M. Quantitative requirements of infant and child for water and electrolytes under varying conditions. Am J Clin Pathol 1953231133–1141. - PubMed
-
- Darrow D C, Pratt E L. Fluid therapy, relation to tissue composition and expenditure of water and electrolytes. JAMA 1950143432–439. - PubMed
-
- Siegel N J. Fluids, electrolytes and acid‐base. In: Rudolph's pediatrics. 21st edn. New York: McGraw Hill, 2003
-
- Greenbaum L A. Pathophysiology of body fluids and fluid therapy. In: Nelson's textbook of pediatrics. 17th edn. Philadelphia: W.B. Saunders, 2004
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous