

Effectiveness of nebulizer use-targeted asthma education on underserved children with asthma
- PMID: 16754825
- PMCID: PMC2269706
- DOI: 10.1001/archpedi.160.6.622
Effectiveness of nebulizer use-targeted asthma education on underserved children with asthma
Abstract
Objective: To determine the effectiveness of a home-based asthma education intervention in increasing appropriate nebulizer use and reducing symptom frequency, emergency department (ED) visits, and hospitalizations over 12 months.
Design: A randomized clinical trial. Settings Pediatric primary care, pulmonary/allergy, and ED practices associated with the University of Maryland Medical System and The Johns Hopkins Hospital, Baltimore.
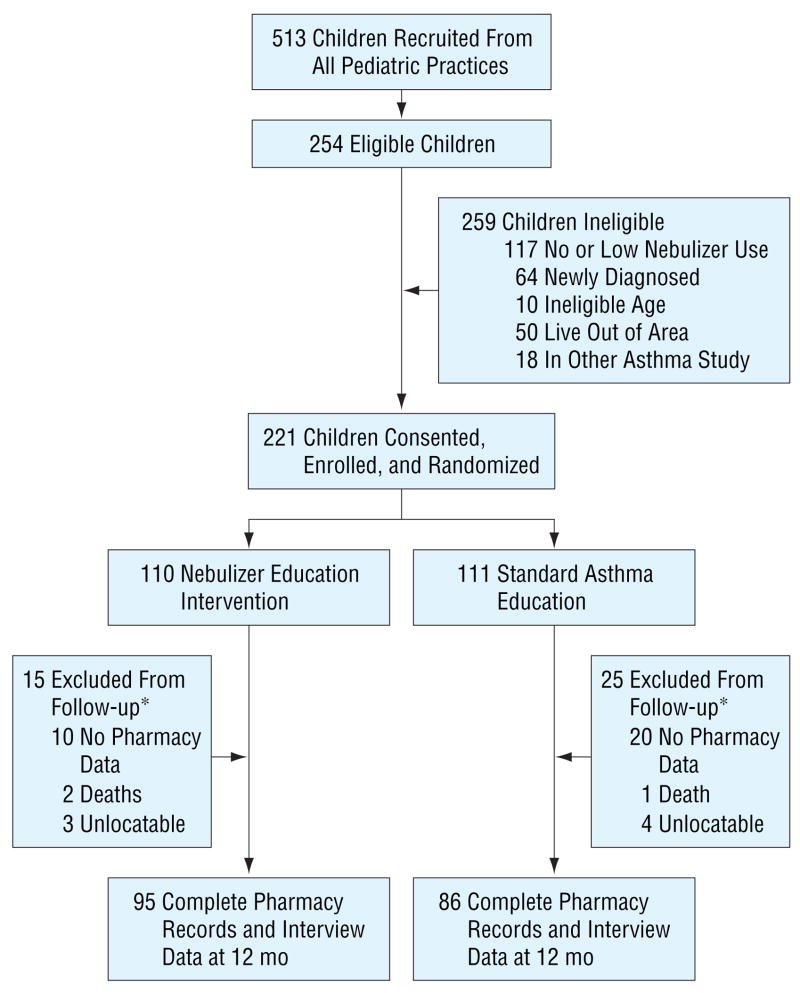
Participants: Children with persistent asthma, aged 2 to 9 years, with regular nebulizer use and an ED visit or hospitalization within the past 12 months. Children were randomized into the intervention (n = 110) or control (n = 111) group. Follow-up data were available for 95 intervention and 86 control children.
Intervention: Home-based asthma education, including symptom recognition, home treatment of acute symptoms, appropriate asthma medication, and nebulizer practice.
Main outcome measures: Estimates of mean differences in asthma symptom frequency, number of ED visits and hospitalizations and appropriate quick relief, controller medication, and nebulizer practice over 12 months.
Results: Of the 221 children, 181 (81.9%) completed the study. There were no significant differences in home nebulizer practice, asthma morbidity, ED visits, or hospitalizations between groups (P range, .11-.79). Although most children received appropriate nonurgent asthma care (mean, 2 visits per 6 months), more than one third of all children received at least 6 quick-relief medication prescriptions during 12 months, with no difference by group.
Conclusions: A nebulizer education intervention had no effect on asthma severity or health care use. Of concern is the high quick-relief and low controller medication use in young children with asthma seen nearly every 3 months for nonurgent care.
Figures
References
-
- American Lung Association Epidemiology and Statistics Unit. Trends in Asthma Morbidity and Mortality. New York, NY: American Lung Association; 2005. pp. 14–16.
-
- National Center for Health Statistics, Centers for Disease Control and Prevention. Health data for all ages. [Accessed October 20, 2005]. Available at: http://www.cdc.gov/NCHS/Healthdataforallages.htm.
-
- Mannino DM, Homa DM, Akinbami LJ, Moorman JE, Gwynn C, Redd SC. Surveillance for asthma: United States, 1980–1999. MMWR Surveill Summ. 2002;51:1–13. - PubMed
-
- Yoos HL, Kitzman H, McMullen A, Sidora K. Symptom perception in childhood asthma: how accurate are children and parents? J Asthma. 2003;40:27–39. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
