

The Canadian Hypertension Education Program--a unique Canadian initiative
- PMID: 16755310
- PMCID: PMC2560862
- DOI: 10.1016/s0828-282x(06)70277-x
The Canadian Hypertension Education Program--a unique Canadian initiative
Abstract
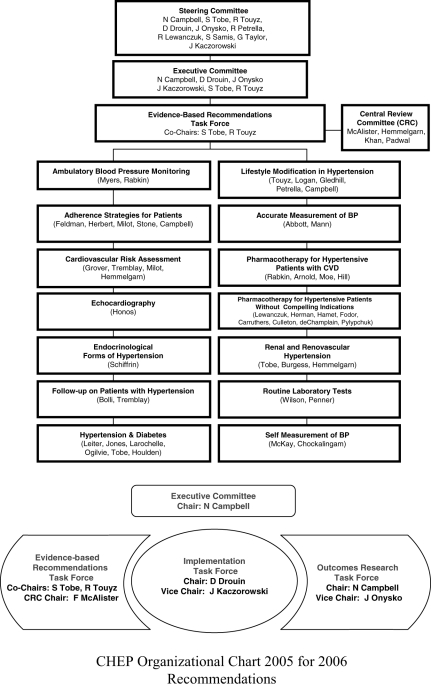
While almost two-thirds of all strokes and one-half of all myocardial infarctions could be prevented if hypertensive individuals had their blood pressures optimally controlled, only a minority of hypertensive individuals (even in publicly funded health care systems with subsidization of medication costs) achieve target blood pressures. Traditional hypertension guidelines have had limited impact on hypertension management and control rates. As a result, the Canadian Hypertension Education Program was developed to address the perceived flaws in the traditional hypertension guideline approach. In the present article, the key features of the Canadian Hypertension Education Program methodology are reviewed, with attention to those factors thought to be critical to the successful translation of recommendations into practice.
Presque les deux tiers des accidents vasculaires cérébraux et la moitié des infarctus du myocarde pourraient être évités si seulement la pression artérielle était bien maîtrisée chez les patients hypertendus; à l’inverse, seule une minorité de personnes hypertendues (même dans les systèmes publics de santé dotés d’un régime de médicaments subventionné) réussissent à atteindre les valeurs cibles de la pression artérielle. Force est de reconnaître que les anciennes lignes directrices ont une faible incidence sur la prise en charge de l’hypertension et sur la normalisation des valeurs. Le Programme d’éducation canadien sur l’hypertension a donc été élaboré dans l’optique de combler les lacunes perçues dans l’ancienne approche. Le présent article porte sur les principaux éléments du Programme et, en particulier, sur les facteurs que l’on croit essentiels à l’application concrète des recommandations.
Figures

References
-
- Joffres MR, Ghadirian P, Fodor JG, Petrasovits A, Chockalingam A, Hamet P. Awareness, treatment, and control of hypertension in Canada. Am J Hypertens. 1997;10:1097–102. - PubMed
-
- Vasan R, Beiser A, Seshadri S, et al. Residual lifetime risk for developing hypertension in middle-aged women and men. The Framingham Heart Study. JAMA. 2002;287:1003–10. - PubMed
-
- Yusuf S, Hawken S, Ounpuu S, et al. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): Case-control study. Lancet. 2004;364:937–52. - PubMed
-
- Kannel WB. Blood pressure as a cardiovascular risk factor: Prevention and treatment. JAMA. 1996;275:1571–6. - PubMed
-
- Ezzati M, Lopez AD, Rodgers A, Vander Hoorn S, Murrary CJ Comparative Risks Assessment Collaborating Group. Selected major risk factors and global and regional burden of disease. Lancet. 2002;360:1347–60. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
