

The role of global risk assessment in hypertension therapy
- PMID: 16755316
- PMCID: PMC2560869
- DOI: 10.1016/s0828-282x(06)70283-5
The role of global risk assessment in hypertension therapy
Abstract
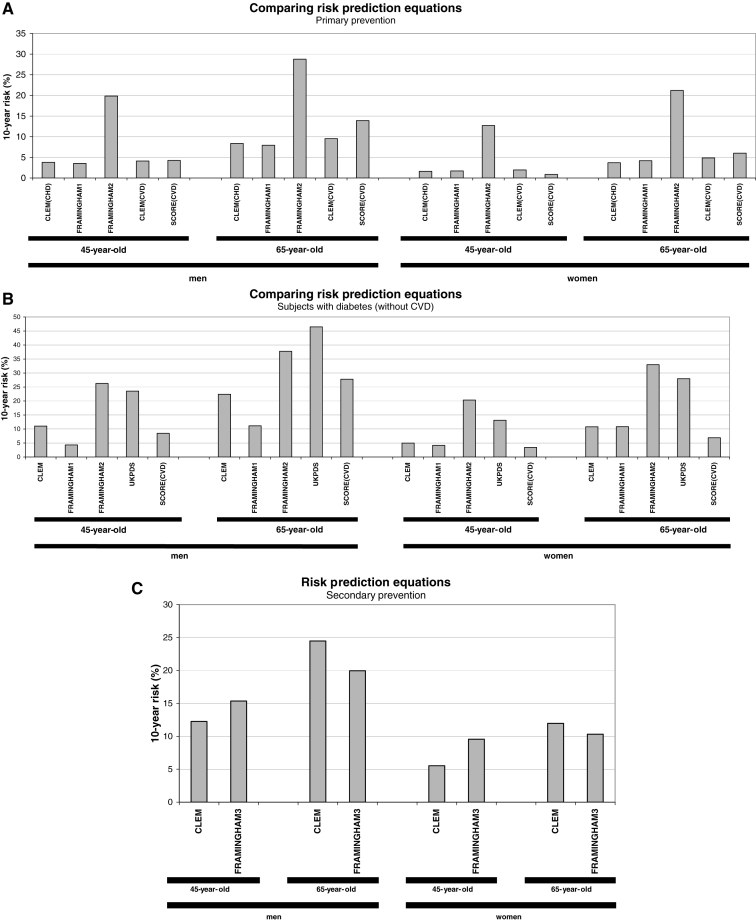
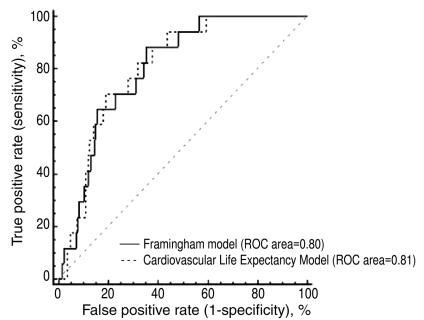
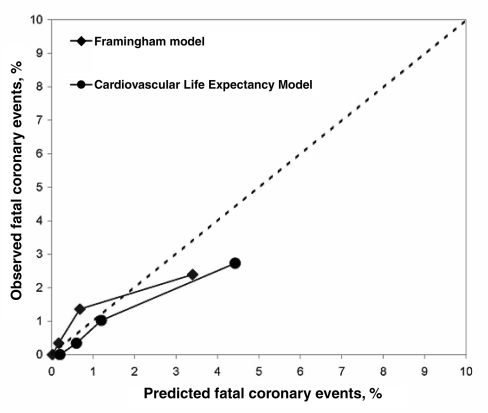
To maximize the benefits of preventive therapy, lipid and hypertension guidelines increasingly recommend that high-risk individuals be targeted for treatment. An individual's risk of developing cardiovascular disease depends on many risk factors, such as age, sex, blood pressure, blood lipid levels, body weight, physical fitness, smoking habits and familial predisposition. Multivariable statistical models have therefore been developed to better estimate the global risk of future coronary events and stroke. A Canadian model is not currently available because a prospective cohort of sufficient size has not been followed in Canada. Therefore, global risk assessment among Canadians can only be completed using models developed in the United States or Europe. In the present review, cardiovascular risk tools are identified that may be appropriate for Canadians, including those based on the Framingham model, the Cardiovascular Life Expectancy Model, the United Kingdom Prospective Diabetes Study (UKPDS) model and the Systematic COronary Risk Evaluation (SCORE) model. The accuracy of the Framingham model and the Cardiovascular Life Expectancy Model are also evaluated using data from a small, prospective Canadian cohort. Finally, a framework is proposed to assist health care professionals in choosing the global risk tool most appropriate for their patients.
Pour maximiser les bienfaits de la thérapie préventive, les lignes directrices sur la lipidémie et l’hypertension recommandent de plus en plus de cibler les personnes très vulnérables pour les traiter. Le risque personnel de souffrir d’une maladie cardiovasculaire dépend de nombreux facteurs de risque, tels que l’âge, le sexe, la tension artérielle, le taux de lipides sanguins, le poids, la condition physique, les habitudes reliées au tabagisme et les prédispositions familiales. Des modèles statistiques multivariables ont donc été mis au point pour mieux évaluer le risque global de futurs problèmes coronariens et accidents vasculaires cérébraux. Il n’existe pas de modèle canadien parce qu’aucune cohorte de taille suffisante n’a été suivie au Canada. Par conséquent, l’évaluation globale du risque chez les Canadiens ne peut être effectuée qu’à l’aide de modèles mis au point aux États-Unis ou en Europe. Dans la présente analyse, les outils de risque cardiovasculaire susceptibles de convenir aux Canadiens sont présentés, soit ceux qui se fondent sur le modèle de Framingham, le modèle d’espérance de vie cardiovasculaire, le modèle de l’étude prospective UKPDS sur le diabète au Royaume-Uni et le modèle SCORE d’évaluation systématique du risque coronarien. L’exactitude du modèle de Framingham et du modèle d’espérance de vie cardiovasculaire est évaluée à l’aide de données tirées d’une petite cohorte canadienne prospective. Enfin, une structure est proposée afin d’aider les professionnels de la santé à choisir l’outil de risque global qui convient le mieux à leur patient.
Figures
References
-
- Anderson KM, Wilson PW, Odell PM, Kannel WB. An updated coronary risk profile. A statement for health professionals. Circulation. 1991;83:356–62. - PubMed
-
- Grover SA, Paquet S, Levinton C, Coupal L, Zowall H. Estimating the benefits of modifying risk factors of cardiovascular disease: A comparison of primary vs secondary prevention. Arch Intern Med. 1998;158:655–62. - PubMed
-
- Heiss G, Tamir I, Davis CE, et al. Lipoprotein-cholesterol distributions in selected North American populations: The lipid research clinics program prevalence study. Circulation. 1980;61:302–15. - PubMed
-
- D’Agostino RB, Sr, Grundy S, Sullivan LM, Wilson P. CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: Results of a multiple ethnic groups investigation. JAMA. 2001;286:180–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
