

Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction
- PMID: 16757723
- PMCID: PMC1782030
- DOI: 10.1001/jama.295.21.2511
Early revascularization and long-term survival in cardiogenic shock complicating acute myocardial infarction
Abstract
Context: Cardiogenic shock remains the major cause of death for patients hospitalized with acute myocardial infarction (MI). Although survival in patients with cardiogenic shock complicating acute MI has been shown to be significantly higher at 1 year in those receiving early revascularization vs initial medical stabilization, data demonstrating long-term survival are lacking.
Objective: To determine if early revascularization affects long-term survival of patients with cardiogenic shock complicating acute MI.
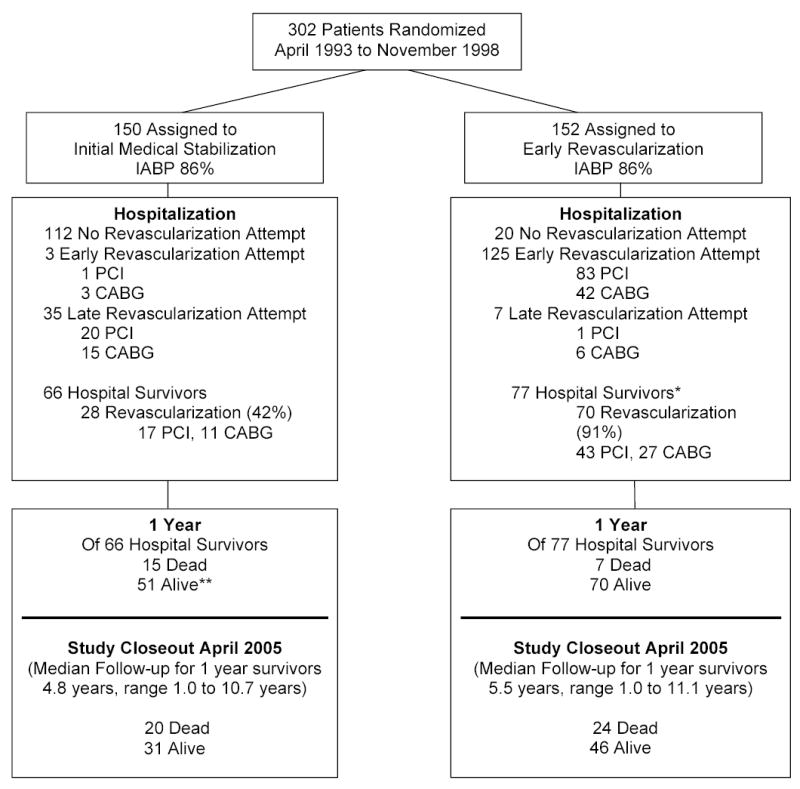
Design, setting, and patients: The Should We Emergently Revascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) trial, an international randomized clinical trial enrolling 302 patients from April 1993 through November 1998 with acute myocardial infarction complicated by cardiogenic shock (mean [SD] age at randomization, 66 [11] years); long-term follow-up of vital status, conducted annually until 2005, ranged from 1 to 11 years (median for survivors, 6 years).
Main outcome measures: All-cause mortality during long-term follow-up.
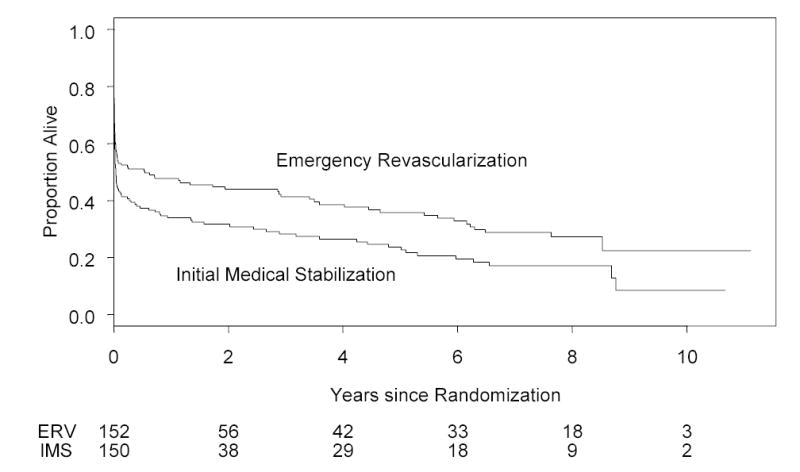
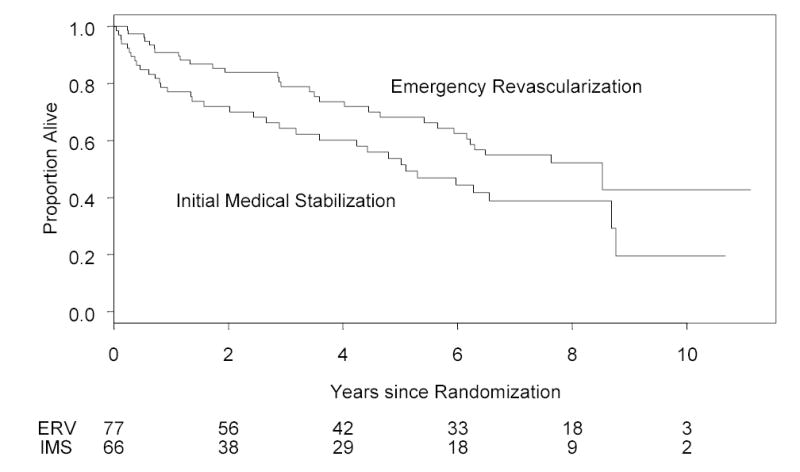
Results: The group difference in survival of 13 absolute percentage points at 1 year favoring those assigned to early revascularization remained stable at 3 and 6 years (13.1% and 13.2%, respectively; hazard ratio [HR], 0.74; 95% confidence interval [CI], 0.57-0.97; log-rank P = .03). At 6 years, overall survival rates were 32.8% and 19.6% in the early revascularization and initial medical stabilization groups, respectively. Among the 143 hospital survivors, a group difference in survival also was observed (HR, 0.59; 95% CI, 0.36-0.95; P = .03). The 6-year survival rates for the hospital survivors were 62.4% vs 44.4% for the early revascularization and initial medical stabilization groups, respectively, with annualized death rates of 8.3% vs 14.3% and, for the 1-year survivors, 8.0% vs 10.7%. There was no significant interaction between any subgroup and treatment effect.
Conclusions: In this randomized trial, almost two thirds of hospital survivors with cardiogenic shock who were treated with early revascularization were alive 6 years later. A strategy of early revascularization resulted in a 13.2% absolute and a 67% relative improvement in 6-year survival compared with initial medical stabilization. Early revascularization should be used for patients with acute MI complicated by cardiogenic shock due to left ventricular failure.
Trial registration: clinicaltrials.gov Identifier: NCT00000552.
Figures
Comment in
-
Early revascularization improved long-term survival after myocardial infarction with cardiogenic shock.ACP J Club. 2006 Nov-Dec;145(3):59. ACP J Club. 2006. PMID: 17080971 No abstract available.
References
-
- Babaev A, Frederick PD, Pasta DJ, et al. Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA. 2005;294:448–54. - PubMed
-
- Goldberg RJ, Gore JM, Alpert JS, et al. Cardiogenic shock after acute myocardial infarction. Incidence and mortality from a community-wide perspective, 1975–1988. N Engl J Med. 1991;325:1117–22. - PubMed
-
- Goldberg RJ, Samad NA, Yarzebski J, et al. Temporal trends in cardiogenic shock complicating acute myocardial infarction. N Engl J Med. 1999;340:1162–8. - PubMed
-
- Becker RC, Gore JM, Lambrew C, et al. A composite view of cardiac rupture in the United States National Registry of Myocardial Infarction. J Am Coll Cardiol. 1996;27:1321–6. - PubMed
-
- Hochman JS, Sleeper LA, Webb JG, et al. Early revascularization in acute myocardial infarction complicated by cardiogenic shock. N Engl J Med. 1999;341:625–34. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
