

Modeling of the temporal patterns of fluoxetine prescriptions and suicide rates in the United States
- PMID: 16768544
- PMCID: PMC1475655
- DOI: 10.1371/journal.pmed.0030190
Modeling of the temporal patterns of fluoxetine prescriptions and suicide rates in the United States
Abstract
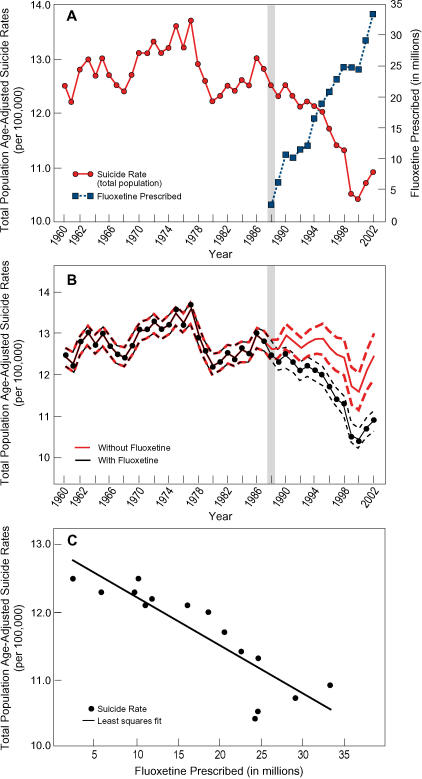
Background: To study the potential association of antidepressant use and suicide at a population level, we analyzed the associations between suicide rates and dispensing of the prototypic SSRI antidepressant fluoxetine in the United States during the period 1960-2002.
Methods and findings: Sources of data included Centers of Disease Control and US Census Bureau age-adjusted suicide rates since 1960 and numbers of fluoxetine sales in the US, since its introduction in 1988. We conducted statistical analysis of age-adjusted population data and prescription numbers. Suicide rates fluctuated between 12.2 and 13.7 per 100,000 for the entire population from the early 1960s until 1988. Since then, suicide rates have gradually declined, with the lowest value of 10.4 per 100,000 in 2000. This steady decline is significantly associated with increased numbers of fluoxetine prescriptions dispensed from 2,469,000 in 1988 to 33,320,000 in 2002 (r(s) = -0.92; p < 0.001). Mathematical modeling of what suicide rates would have been during the 1988-2002 period based on pre-1988 data indicates that since the introduction of fluoxetine in 1988 through 2002 there has been a cumulative decrease in expected suicide mortality of 33,600 individuals (posterior median, 95% Bayesian credible interval 22,400-45,000).
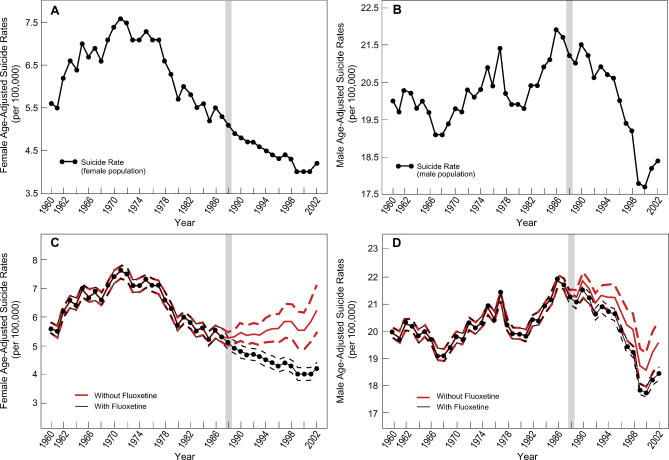
Conclusions: The introduction of SSRIs in 1988 has been temporally associated with a substantial reduction in the number of suicides. This effect may have been more apparent in the female population, whom we postulate might have particularly benefited from SSRI treatment. While these types of data cannot lead to conclusions on causality, we suggest here that in the context of untreated depression being the major cause of suicide, antidepressant treatment could have had a contributory role in the reduction of suicide rates in the period 1988-2002.
Conflict of interest statement
Figures

Comment in
-
Is it just a marker for increased care?PLoS Med. 2006 Sep;3(9):e406; author reply e407. doi: 10.1371/journal.pmed.0030406. PLoS Med. 2006. PMID: 17002507 Free PMC article. No abstract available.
-
Were Eli Lilly unaware of this study?PLoS Med. 2006 Sep;3(9):e408; author reply e407. doi: 10.1371/journal.pmed.0030408. PLoS Med. 2006. PMID: 17002509 Free PMC article. No abstract available.
-
Fluoxetine and suicide rates: suicide and the economy.PLoS Med. 2006 Nov;3(11):e501; author reply e504. doi: 10.1371/journal.pmed.0030501. PLoS Med. 2006. PMID: 17132055 Free PMC article. No abstract available.
References
-
- Isacsson G, Holmgren P, Druid H, Bergman U. Psychotropics and suicide prevention. Implications from toxicological screening of 5281 suicides in Sweden 1992–1994. Br J Psychiatry. 1999;174:259–265. - PubMed
-
- Weissman MM, Bland RC, Canino GJ, Faravelli C, Greenwald S, et al. Cross-national epidemiology of major depression and bipolar disorder. JAMA. 1996;276:293–299. - PubMed
-
- Wong ML, Licinio J. Biology of depression: From novel insights to therapeutic strategies. Weinheim (Germany): Wiley-VCH; 2005. 1092 pp.
-
- Wong ML, Licinio J. From monoamines to genomic targets: A paradigm shift for drug discovery in depression. Nat Rev Drug Discov. 2004;3:136–151. - PubMed
-
- Wong ML, Licinio J. Research and treatment approaches to depression. Nature Rev Neurosci. 2001;2:343–351. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- K12 RR017611/RR/NCRR NIH HHS/United States
- M01 RR000865/RR/NCRR NIH HHS/United States
- MH062777/MH/NIMH NIH HHS/United States
- DK063240/DK/NIDDK NIH HHS/United States
- R03 HG002500/HG/NHGRI NIH HHS/United States
- GM61394/GM/NIGMS NIH HHS/United States
- K30 HL004526/HL/NHLBI NIH HHS/United States
- K24 RR017365/RR/NCRR NIH HHS/United States
- RR16996/RR/NCRR NIH HHS/United States
- K12RR17611/RR/NCRR NIH HHS/United States
- HG002500/HG/NHGRI NIH HHS/United States
- RR000865/RR/NCRR NIH HHS/United States
- R01 DK063240/DK/NIDDK NIH HHS/United States
- RR017365/RR/NCRR NIH HHS/United States
- K30HL04526/HL/NHLBI NIH HHS/United States
- U01 GM061394/GM/NIGMS NIH HHS/United States
- K24 RR016996/RR/NCRR NIH HHS/United States
