

Optimal utilization of donor grafts with extended criteria: a single-center experience in over 1000 liver transplants
- PMID: 16772778
- PMCID: PMC1570573
- DOI: 10.1097/01.sla.0000219669.84192.b3
Optimal utilization of donor grafts with extended criteria: a single-center experience in over 1000 liver transplants
Abstract
Objective: Severely limited organ resources mandate maximum utilization of donor allografts for orthotopic liver transplantation (OLT). This work aimed to identify factors that impact survival outcomes for extended criteria donors (ECD) and developed an ECD scoring system to facilitate graft-recipient matching and optimize utilization of ECDs.
Methods: Retrospective analysis of over 1000 primary adult OLTs at UCLA. Extended criteria (EC) considered included donor age (>55 years), donor hospital stay (>5 days), cold ischemia time (>10 hours), and warm ischemia time (>40 minutes). One point was assigned for each extended criterion. Cox proportional hazard regression model was used for multivariate analysis.
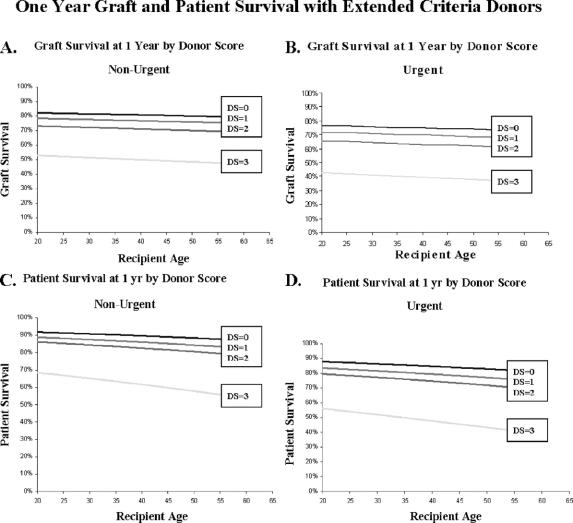
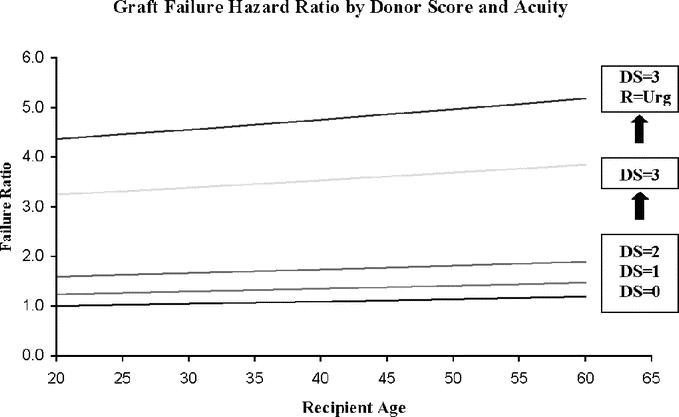
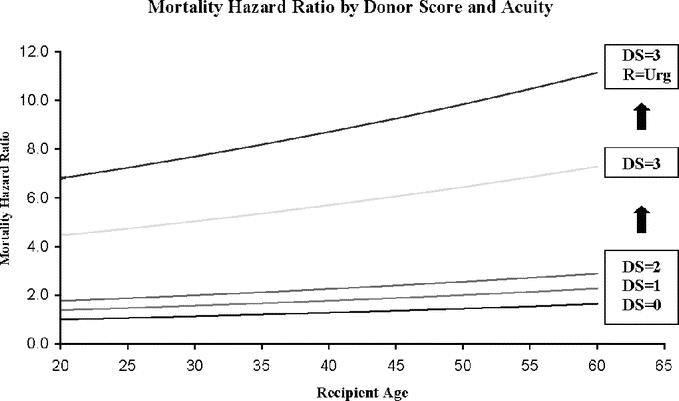
Results: Of 1153 allografts considered in the study, 568 organs exhibited no extended criteria (0 score), while 429, 135 and 21 donor allografts exhibited an EC score of 1, 2 and 3, respectively. Overall 1-year patient survival rates were 88%, 82%, 77% and 48% for recipients with EC scores of 0, 1, 2 and 3 respectively (P < 0.001). Adjusting for recipient age and urgency at the time of transplantation, multivariate analysis identified an ascending mortality risk ratio of 1.4 and 1.8 compared to a score of 0 for an EC score of 1, and 2 (P < 0.01) respectively. In contrast, an EC score of 3 was associated with a mortality risk ratio of 4.5 (P < 0.001). Further, advanced recipient age linearly increased the death hazard ratio, while an urgent recipient status increased the risk ratio of death by 50%.
Conclusions: Extended criteria donors can be scored using readily available parameters. Optimizing perioperative variables and matching ECD allografts to appropriately selected recipients are crucial to maintain acceptable outcomes and represent a preferable alternative to both high waiting list mortality and to a potentially futile transplant that utilizes an ECD for a critically ill recipient.
Figures
References
-
- United Network for Organ Sharing website (www.unos.org), accessed November 2005.
-
- Busuttil RW, Tanaka Koichi. The utility of marginal donors in liver transplantation. Liver Transpl. 2003;9:651–663. - PubMed
-
- Strasberg SM, Howard TK, Molmenti EP, et al. Selecting donor livers: risk factors for poor function after orthotopic liver transplantation. Hepatology. 1994;20:829–838. - PubMed
-
- Mor E, Klintmalm GB, Gonwa TA, et al. The use of marginal donors for liver transplantation: a retrospective study of 365 liver donors. Transplantation. 1992;53:383–386. - PubMed
-
- Freeman R, Weisner RH, Edwards E, et al. Results of the first year of the new liver allocation plan. Liver Transpl. 2004;10:7–15. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
