

Laparoscopic skills are improved with LapMentor training: results of a randomized, double-blinded study
- PMID: 16772789
- PMCID: PMC1570578
- DOI: 10.1097/01.sla.0000219641.79092.e5
Laparoscopic skills are improved with LapMentor training: results of a randomized, double-blinded study
Abstract
Objective: To determine if prior training on the LapMentor laparoscopic simulator leads to improved performance of basic laparoscopic skills in the animate operating room environment.
Summary background data: Numerous influences have led to the development of computer-aided laparoscopic simulators: a need for greater efficiency in training, the unique and complex nature of laparoscopic surgery, and the increasing demand that surgeons demonstrate competence before proceeding to the operating room. The LapMentor simulator is expensive, however, and its use must be validated and justified prior to implementation into surgical training programs.
Methods: Nineteen surgical interns were randomized to training on the LapMentor laparoscopic simulator (n = 10) or to a control group (no simulator training, n = 9). Subjects randomized to the LapMentor trained to expert criterion levels 2 consecutive times on 6 designated basic skills modules. All subjects then completed a series of laparoscopic exercises in a live porcine model, and performance was assessed independently by 2 blinded reviewers. Time, accuracy rates, and global assessments of performance were recorded with an interrater reliability between reviewers of 0.99.
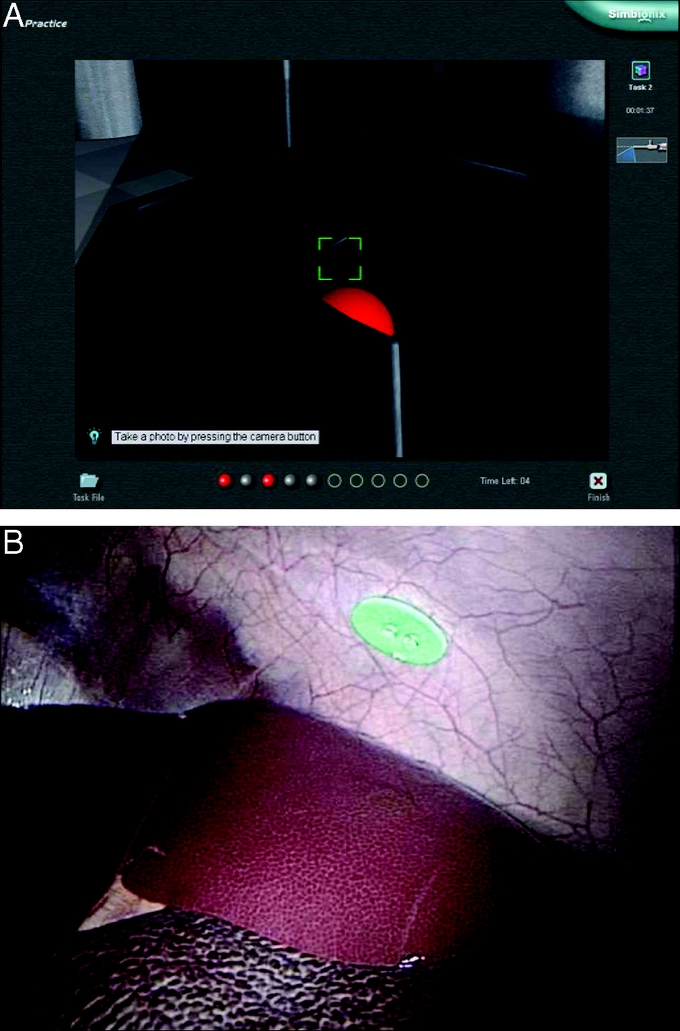
Results: LapMentor trained interns completed the 30 degrees camera navigation exercise in significantly less time than control interns (166 +/- 52 vs. 220 +/- 39 seconds, P < 0.05); they also achieved higher accuracy rates in identifying the required objects with the laparoscope (96% +/- 8% vs. 82% +/- 15%, P < 0.05). Similarly, on the two-handed object transfer exercise, task completion time for LapMentor trained versus control interns was 130 +/- 23 versus 184 +/- 43 seconds (P < 0.01) with an accuracy rate of 98% +/- 5% versus 80% +/- 13% (P < 0.001). Additionally, LapMentor trained interns outperformed control subjects with regard to camera navigation skills, efficiency of motion, optimal instrument handling, perceptual ability, and performance of safe electrocautery.
Conclusions: This study demonstrates that prior training on the LapMentor laparoscopic simulator leads to improved resident performance of basic skills in the animate operating room environment. This work marks the first prospective, randomized evaluation of the LapMentor simulator, and provides evidence that LapMentor training may lead to improved operating room performance.
Figures
References
-
- Ziv A, Wolpe PR, Small SD, et al. Simulation-based medical education: an ethical imperative. Acad Med. 2003;78:783–788. - PubMed
-
- Youngblood PL, Srivastava S, Curet M, et al. Comparison of training on two laparoscopic simulators and assessment of skills transfer to surgical performance. J Am Coll Surg. 2005;200:546–551. - PubMed
-
- Jordan JA, Gallagher AG, McGuigan J, et al. Virtual reality training leads to faster adaptation to the novel psychomotor restrictions encountered by laparoscopic surgeons. Surg Endosc. 2001;15:1080–1084. - PubMed
-
- Fried GM, Derossis AM, Bothwell J, et al. Comparison of laparoscopic performance in vivo with performance measured in a laparoscopic simulator. Surg Endosc. 1999;13:1077–1081; discussion 1082. - PubMed
-
- Hyltander A, Liljegren E, Rhodin PH, et al. The transfer of basic skills learned in a laparoscopic simulator to the operating room. Surg Endosc. 2002;16:1324–1328. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
