

Short-term and long-term outcomes in 133,429 emergency patients admitted with angina or myocardial infarction in Scotland, 1990-2000: population-based cohort study
- PMID: 16775090
- PMCID: PMC1861246
- DOI: 10.1136/hrt.2005.085399
Short-term and long-term outcomes in 133,429 emergency patients admitted with angina or myocardial infarction in Scotland, 1990-2000: population-based cohort study
Abstract
Objective: To analyse short- and long-term outcomes and prognostic factors in a large population-based cohort of unselected patients with a first emergency admission for suspected acute coronary syndrome between 1990 and 2000 in Scotland.
Methods: All first emergency admissions for acute myocardial infarction (AMI) and all first emergency admissions for angina (the proxy for unstable angina) between 1990 and 2000 in Scotland (population 5.1 million) were identified. Survival to five years was examined by Cox multivariate modelling to examine the independent prognostic effects of diagnosis, age, sex, year of admission, socioeconomic deprivation and co-morbidity.
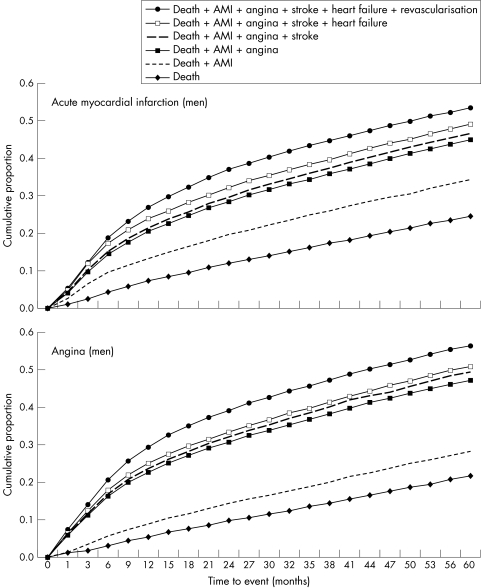
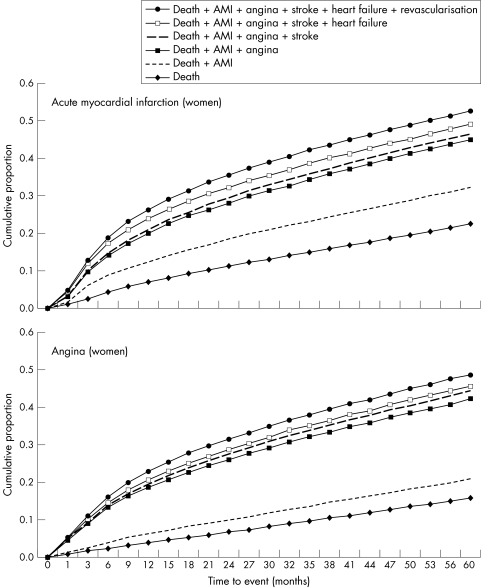
Results: In Scotland between 1990 and 2000, 133,429 individual patients had a first emergency admission for suspected acute coronary syndrome: 96 026 with AMI and 37,403 with angina. After exclusion of deaths within 30 days, crude five-year case fatality was similarly poor for patients with angina and those with AMI (23.9% v 21.6% in men and 23.5% v 26.0% in women). The longer-term risk of a subsequent fatal or non-fatal event in the five years after first hospital admission was high: 54% in men after AMI (53% in women) and 56% after angina (49% in women). Event rates increased threefold with increasing age and 20-60% with different co-morbidities, but were 11-34% lower in women.
Conclusions: Longer-term case fatality was similarly high in patients with angina and in survivors of AMI, about 5% a year. Furthermore, half the patients experienced a fatal or non-fatal event within five years. These data may strengthen the case for aggressive secondary prevention in all patients presenting with acute coronary syndrome.
Conflict of interest statement
Competing interests: None declared.
References
-
- British Heart Foundation British Heart Foundation Statistics Website. Hospitalisations. http://www.heartstats.org/datapage.asp?id = 842 (accessed 14 Jun 2005)
-
- Davie A P, Caesar D, Caruana L.et al Outcome from a rapid‐assessment chest pain clinic: closing Pandora's box? QJM 199891339–343. - PubMed
-
- Braunwald E. Application of current guidelines to the management of unstable angina and non‐ST‐elevation myocardial infarction. Circulation 2003108(16 Suppl 1)III28–III37. - PubMed
-
- Department of Health National Service Framework for Coronary Heart Disease. London: Department of Health, 2000, http://www.dh.gov.uk/PublicationsAndStatistics/Publications/Publications... = 4105281&chk = HmsiOz (accessed 14 Jun 2005)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical