

Review
Multiple sclerosis: the role of MR imaging
Affiliations
- PMID: 16775258
- PMCID: PMC8133908
Item in Clipboard
Review
Multiple sclerosis: the role of MR imaging
AJNR Am J Neuroradiol.
2006 Jun-Jul.
Abstract
MR offers by far the most sensitive technique for detecting multiple sclerosis (MS) lesions and has proved to be an important paraclinical tool for diagnosing MS and monitoring therapeutic trials. Technologic advances of MR in recent years have dramatically improved our understanding of MS disease. This review will focus on the contribution of MR imaging in MS and provide a discussion of conventional and advanced nonconventional MR techniques with regard to current findings, clinical correlations, and future directions.
Figures

Axial T2-weighted images of a 43-year-old RRMS patient show prominent perivascular spaces (short arrows), which project radially and are aligned with lesions, following the course and configuration of deep venular structures. This may be associated with perivascular inflammation, which initiates the development of new lesions (long arrow). These prominent perivascular spaces might have implications for differentiating primary from secondary demyelinating lesions.

A 30-year-old female RRMS patient shown on T2WI (A), FLAIR (B), and contrast-enhanced T1WI. The lesions on FLAIR are usually prominent and several small lesions are depicted only on FLAIR (arrows). The lesion enhancement can be nodule (as shown in this case) or ringlike on T1-weighted imaging.

MS lesion (arrow) in corpus callosum on FLAIR imaging is failed to be picked up on T2-weighted imaging.

Averaged magnetization transfer ratio histograms from 3 groups (healthy control, RRMS, and SPMS) for global NAGM (A) and NAWM (B) tissues. Lower normalized peak height in SPMS population indicates relatively less residual normal brain tissue compared with that in RRMS patients.

DTI (left, b = 0), FA (middle), and MD (right) maps of a 31-year-old female patient with RRMS. The decreased value of FA and increased value of MD for the lesions (arrows) are shown in their maps. Note that the decreased FA (arrowhead) in some white matter areas is probably due to fiber crossing.

Fiber tractography in a patient with MS (A) and a healthy volunteer (B). All the MS plaques (arrows) were marked and constructed in 3D. Note the reduced number of fibers when they traverse white matter lesions in the patient.
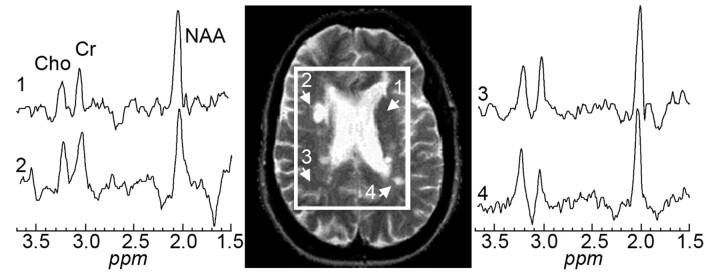
Axial T2-weighed (TE/TR = 90/2500 msec) image of a 26-year-old woman MS patient superimposed with the MR spectroscopy volume of interest. Spectra from 2 lesions (2 and 4) and 2 contralateral NAWM regions (1 and 3) are shown on common intensity and chemical shift (ppm) scales.

Axial gradient-echo imaging in a 29-year-old patient with MS (A) and a 34-year-old healthy volunteer (B). Greater hypointense signal intensities, which may be associated with excessive iron deposition, are seen in all ferruginated neurons in a patient compared with a healthy volunteer.
References
-
- Adams CW, Abdulla YH, Torres EM, et al. Periventricular lesions in multiple sclerosis: their perivenous origin and relationship to granular ependymitis. Neuropathol Appl Neurobiol 1987;13:141–52 - PubMed
-
- Paolillo A, Giugni E, Bozzao A, et al. [Fast spin echo and fast fluid attenuated inversion recovery sequences in multiple sclerosis]. Radiol Med (Torino) 1997;93:686–91 - PubMed
-
- Bo L, Vedeler CA, Nyland H, et al. Intracortical multiple sclerosis lesions are not associated with increased lymphocyte infiltration. Mult Scler 2003;9:323–31 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical