

Transjugular intrahepatic portosystemic shunt before abdominal surgery in cirrhotic patients: a retrospective, comparative study
- PMID: 16779457
- PMCID: PMC2659922
- DOI: 10.1155/2006/245082
Transjugular intrahepatic portosystemic shunt before abdominal surgery in cirrhotic patients: a retrospective, comparative study
Abstract
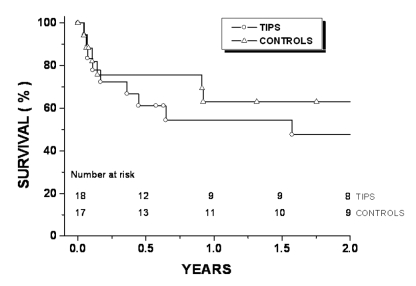
Surgery in cirrhotic patients is associated with high morbidity and mortality related to portal hypertension and liver insufficiency. Therefore, preoperative portal decompression is a logical approach to facilitate abdominal surgery and hopefully to improve postoperative survival. The present study evaluated the clinical outcomes of 18 patients (mean age 58 years) with cirrhosis (seven alcoholics and 11 nonalcoholics) who underwent transjugular intrahepatic portosystemic shunt (TIPS) placement before antrectomy (n=5), colectomy (n=10), small-bowel resection (n=1), pancreatectomy (n=1) and nephrectomy (n=1). TIPS was performed a mean (+/-SD) of 72+/-21 days before surgery and induced a marked mean decrease in portohepatic gradient from 21.4+/-3.9 mmHg to 8.4+/-3.4 mmHg. Cirrhotic patients (n=17) who underwent elective abdominal surgery without preoperative TIPS placement were used as the control group. Both groups were matched for age, etiology of cirrhosis, indications for surgery, type of surgery and coagulation parameters. The mean Pugh score was significantly higher in the TIPS group (7.7 versus 6.2). No significant differences were observed for operative blood loss, postoperative complications, duration of hospitalization and one-month (83% versus 88%) or one-year (54% versus 63%) cumulative survival rate. Analysis using the Cox proportional hazards model showed that neither TIPS placement nor preoperative Pugh score were independent predictors for survival. The present study suggests that preoperative TIPS placement does not improve postoperative evolution after abdominal surgery in cirrhotic patients with good or moderately impaired liver function.
Les interventions chirurgicales chez les patients cirrhotiques s’associent à des taux élevés de morbidité et de mortalité reliés à l’hypertension portale et à l’insuffisance hépatique. Par conséquent, la décompression portale préopératoire constitue une démarche logique afin de faciliter une opération abdominale et, si tout va bien, d’améliorer la survie postopératoire. La présente étude a permis d’évaluer les issues cliniques de 18 patients (âge moyen de 58 ans) cirrhotiques (sept alcooliques et 11 non-alcooliques) qui avaient subi une dérivation transjugulaire intrahépatique portosystémique (DTIP) avant une antrectomie (n=5), une colectomie (n=10), une résection de l’intestin grêle (n=1), une pancréatectomie (n=1) et une néphrectomie (n=1). La DTIP a été exécutée en moyenne (±ÉT) 72±21 jours avant l’opération et a induit une diminution moyenne marquée du gradient portohépatique, qui est passé de 21,4±3,9 mmHg à 8,4±3,4 mmHg. Des patients cirrhotiques (n=17) qui avaient subi une intervention abdominale non urgente sans DTIP préopératoire ont servi de groupe témoin. Les deux groupes étaient appariés selon l’âge, l’étiologie de la cirrhose, les indications d’opérer, le type d’opération et les paramètres de coagulation. L’indice de Pugh moyen étaient considérablement plus élevé au sein du groupe ayant subi la DTIP (7,7 par rapport à 6,2). On n’a remarqué aucune différence significative pour ce qui est de la perte de sang opératoire, des complications postopératoires, de la durée de l’hospitalisation et du taux de survie cumulatif au bout d’un mois (83 % par rapport à 88 %) ou d’un an (54 % par rapport à 63 %). L’analyse au moyen du modèle des hasards proportionnels de Cox a démontré que ni la DTIP ni l’indice de Pugh préopératoire n’étaient des prédicteurs indépendants de survie. D’après la présente étude, la DTIP préopératoire n’améliore pas l’évolution postopératoire après une intervention abdominale chez des patients cirrhotiques dont la fonction hépatique est bonne ou modérément atteinte.
Figures
Similar articles
-
Cirrhotic patients with a transjugular intrahepatic portosystemic shunt undergoing major extrahepatic surgery.J Clin Gastroenterol. 2009 Jul;43(6):574-9. doi: 10.1097/MCG.0b013e31818738ef. J Clin Gastroenterol. 2009. PMID: 19169145
-
Transjugular intrahepatic portosystemic shunt placement before abdominal intervention in cirrhotic patients with portal hypertension: lessons from a pilot study.Eur J Gastroenterol Hepatol. 2018 Jan;30(1):21-26. doi: 10.1097/MEG.0000000000000990. Eur J Gastroenterol Hepatol. 2018. PMID: 29049129
-
Transjugular intrahepatic portosystemic shunt placement increases feasibility of colorectal surgery in cirrhotic patients with severe portal hypertension.Dig Liver Dis. 2015 Jan;47(1):81-4. doi: 10.1016/j.dld.2014.09.013. Epub 2014 Oct 18. Dig Liver Dis. 2015. PMID: 25445406
-
A systematic review of preoperative transjugular intrahepatic portosystemic shunt prior to extrahepatic, abdominal surgery in patients with cirrhosis.Saudi J Gastroenterol. 2024 Sep 1;30(5):275-282. doi: 10.4103/sjg.sjg_114_24. Epub 2024 Jun 24. Saudi J Gastroenterol. 2024. PMID: 38916207 Free PMC article.
-
Transjugular intrahepatic portosystemic shunt as a bridge to non-hepatic surgery in cirrhotic patients with severe portal hypertension: a systematic review.HPB (Oxford). 2018 Feb;20(2):101-109. doi: 10.1016/j.hpb.2017.09.006. Epub 2017 Oct 27. HPB (Oxford). 2018. PMID: 29110990
Cited by
-
TIPSS as a bridge to extrahepatic abdominal surgery: a case report.Oxf Med Case Reports. 2022 Apr 19;2022(4):omac029. doi: 10.1093/omcr/omac029. eCollection 2022 Apr. Oxf Med Case Reports. 2022. PMID: 35464893 Free PMC article.
-
Impact of transjugular intrahepatic portosystemic shunt on post-colectomy complications in patients with ulcerative colitis and primary sclerosing cholangitis.Gastroenterol Rep (Oxf). 2015 Aug;3(3):228-33. doi: 10.1093/gastro/gou085. Epub 2014 Dec 16. Gastroenterol Rep (Oxf). 2015. PMID: 25519485 Free PMC article.
-
Impact of pre-operative transjugular intrahepatic portosystemic shunt on post-operative outcomes following non-transplant surgeries in patients with decompensated cirrhosis.Transl Gastroenterol Hepatol. 2023 Jan 25;8:9. doi: 10.21037/tgh-21-133. eCollection 2023. Transl Gastroenterol Hepatol. 2023. PMID: 36704652 Free PMC article.
-
Management of Decompensated Cirrhosis in the Surgical ICU: an American Association for the Surgery of Trauma Critical Care Committee Clinical Consensus Document.Trauma Surg Acute Care Open. 2022 Aug 1;7(1):e000936. doi: 10.1136/tsaco-2022-000936. eCollection 2022. Trauma Surg Acute Care Open. 2022. PMID: 35991906 Free PMC article.
-
Surgical Risk Assessment in Patients with Chronic Liver Diseases.J Clin Exp Hepatol. 2022 Jul-Aug;12(4):1175-1183. doi: 10.1016/j.jceh.2022.03.004. Epub 2022 Mar 23. J Clin Exp Hepatol. 2022. PMID: 35814505 Free PMC article. Review.
References
-
- Aranha GV, Greenlee HB. Intra-abdominal surgery in patients with advanced cirrhosis. Arch Surg. 1986;121:275–7. - PubMed
-
- del Olmo JA, Flor-Lorente B, Flor-Civera B, et al. Risk factors for nonhepatic surgery in patients with cirrhosis. World J Surg. 2003;27:647–52. - PubMed
-
- Zarski JP, Richard P, Bourbon P, Demongeot J, Rahail M. Extrahepatic digestive surgery in cirrhotic patients: Mortality, morbidity, preoperative prognostic factors. Gastroenterol Clin Biol. 1988;12:43–7. - PubMed
-
- Boyer TD. Transjugular intrahepatic portosystemic shunt: Current status. Gastroenterology. 2003;124:1700–10. - PubMed
-
- Azoulay D, Buabse F, Damiano I, et al. Neoadjuvant transjugular intrahepatic portosystemic shunt: A solution for extrahepatic abdominal operation in cirrhotic patients with severe portal hypertension. J Am Coll Surg. 2001;193:46–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical