

Self-report measures of antiretroviral therapy adherence: A review with recommendations for HIV research and clinical management
- PMID: 16783535
- PMCID: PMC4083461
- DOI: 10.1007/s10461-006-9078-6
Self-report measures of antiretroviral therapy adherence: A review with recommendations for HIV research and clinical management
Abstract
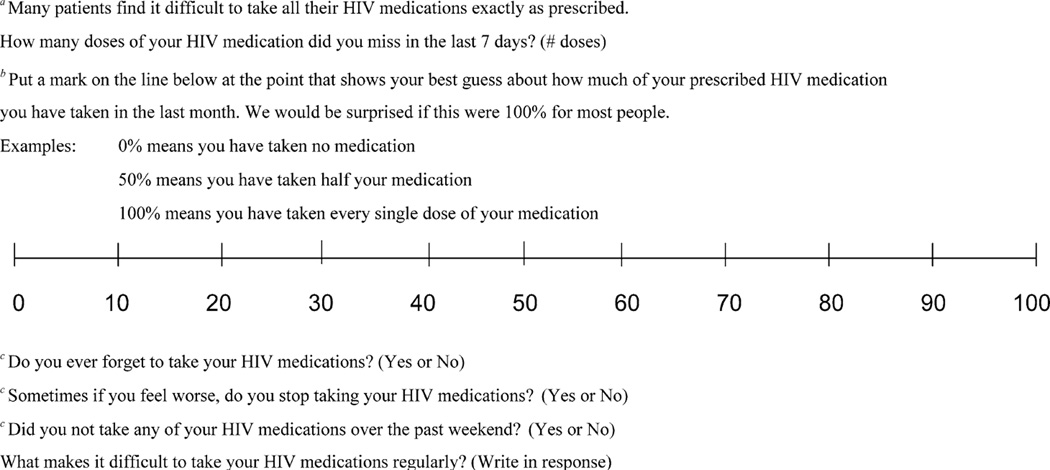
A review of 77 studies employing self-report measures of antiretroviral adherence published 1/1996 through 8/2004 revealed great variety in adherence assessment item content, format, and response options. Recall periods ranged from 2 to 365 days (mode = 7 days). The most common cutoff for optimal adherence was 100% (21/48 studies, or 44%). In 27 of 34 recall periods (79%), self-reported adherence was associated with adherence as assessed with other indirect measures. Data from 57 of 67 recall periods (84%) indicated self-reported adherence was significantly associated with HIV-1 RNA viral load; in 16 of 26 (62%), it was associated with CD4 count. Clearly, the field would benefit from item standardization and a priori definitions and operationalizations of adherence. We conclude that even brief self-report measures of antiretroviral adherence can be robust, and recommend items and strategies for HIV research and clinical management.
Figures

Comment in
-
Utility of self-reported antiretroviral adherence: Comment on Simoni et al. (2006).AIDS Behav. 2006 May;10(3):247-8. doi: 10.1007/s10461-006-9122-6. AIDS Behav. 2006. PMID: 16783536 No abstract available.
References
-
- Alcoba M, Cuevas MJ, Perez-Simon MR, Mostaza JL, Ortega L, Ortiz de Urbina J, et al. Assessment of adherence to triple antiretroviral treatment including indinavir: Role of the determination of plasma levels of indinavir. Journal of Acquired Immune Deficiency Syndromes. 2003;33(2):253–258. - PubMed
-
- Aloisi MS, Arici C, Balzano R, Noto P, Piscopo R, Filice G, et al. Behavioral correlates of adherence to antiretroviral therapy. Journal of Acquired Immune Deficiency Syndromes. 2002;31(Suppl 3):S145–S148. - PubMed
-
- Altice FL, Mostashari F, Friedland GH. Trust and the acceptance of and adherence to antiretroviral therapy. Journal of Acquired Immune Deficiency Syndromes. 2001;28(1):47–58. - PubMed
-
- Ammassari A, Antinori A, Aloisi MS, Trotta MP, Murri R, Bartoli L, et al. Depressive symptoms, neurocognitive impairment, and adherence to highly active antiretroviral therapy among HIV-infected persons. Psychosomatics. 2004;45(5):394–402. - PubMed
-
- Antinori A, Cozzi-Lepri A, Ammassari A, Trotta MP, Nauwelaers D, Hoetelmans R. Relative prognostic value of self-reported adherence and plasma NNRTI/PI concentrations to predict virological rebound in patients initially responding to HAART. Antiviral Therapy. 2004;9(2):291–296. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
