

Review
MCL injuries of the knee: current concepts review
Affiliations
- PMID: 16789454
- PMCID: PMC1888587
Item in Clipboard
Review
MCL injuries of the knee: current concepts review
Iowa Orthop J.
2006.
Abstract
Medial collateral ligament (MCL) injury is one of the most common knee injuries, especially in young athletic patients. Most MCL injuries can be managed conservatively with good results. However, a complete understanding of knee anatomy and the involved structures is necessary to make intelligent treatment decisions. We will review the anatomy and biomechanics of the MCL, classification systems for MCL injuries, and operative and nonoperative treatment for acute and chronic MCL injuries.
Figures
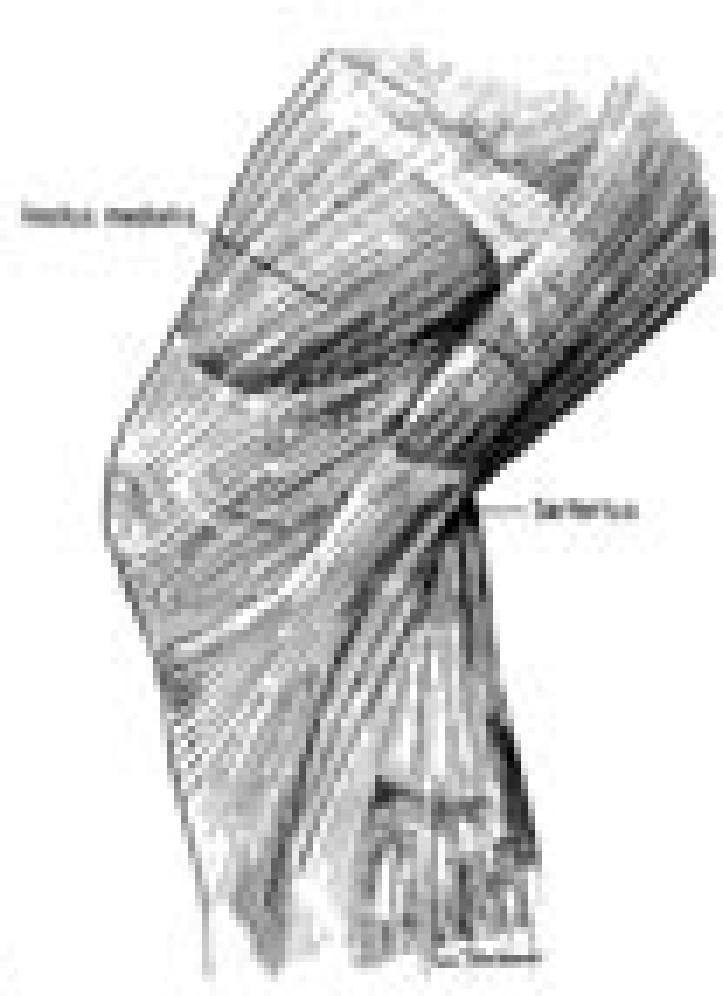
Layer I is the deep crural fascia which is in continuity with the medial patellar retinaculum and the sartorial fascia. The fascia spans from the patellar tendon anteriorly to the midline of the popliteal fossa posteriorly. (From Warren LF, Marshall JL. The supporting structures and layers on the medial side of the knee, an anatomic analysis. J Bone Joint Surg Am 1979;61:58, permission granted.)
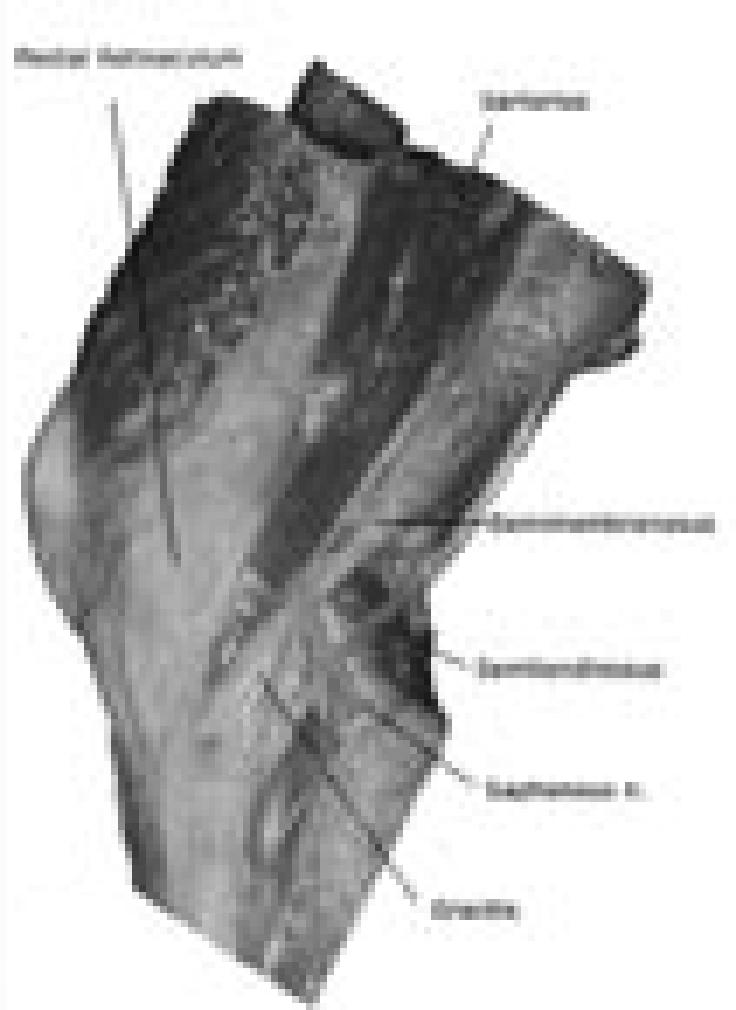
A cadaver dissection reveals the relationship of the medial retinaculum, the pes anserinus tendons, the semimembranosus tendon, and the saphenous nerve.
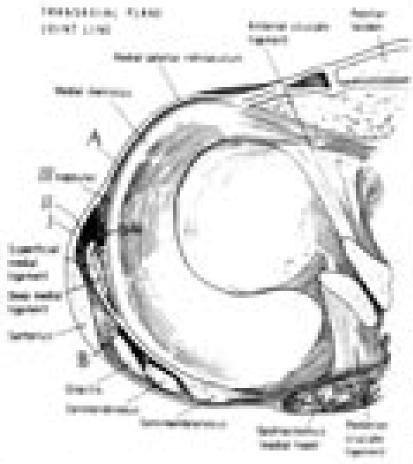
Cross-section anatomy at the level of the joint line is demonstrated. A split can be seen just in front of the superficial MCL. Layer I and II blend together along a vertical line 1-2 cm anterior to the anterior border of the superficial MCL. At the posteromedial corner of the knee, layers II and III merge forming the posterior oblique ligament, which is augmented by the insertion of the semimembranosus insertions. (From Warren LF, Marshall JL. The supporting structures and layers on the medial side of the knee, an anatomic analysis. J Bone Joint Surg Am 1979;61:58, permission granted.)
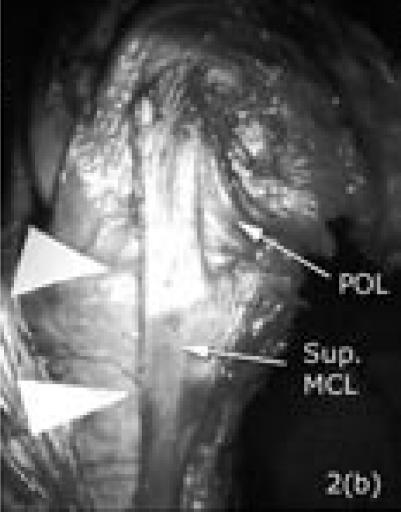
A cadaver dissection shows the slit in front of the superficial MCL (two white triangles). The ligament is long and inserts about 5-7 cm below the joint line. The posterior oblique ligament (POL) is clearly shown in continuity with the parallel fibers of the superficial MCL posteriorly.
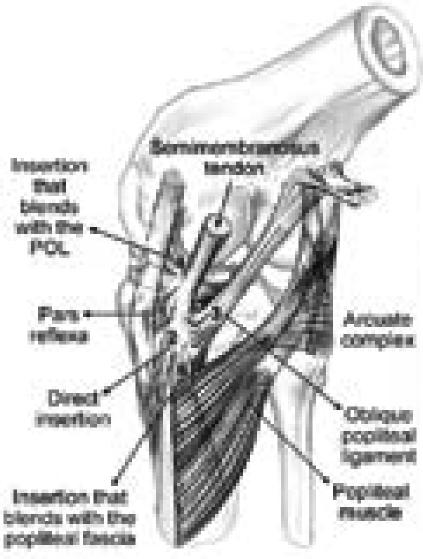
The posteromedial structures of the knee are demonstrated. Note the relationship between the posterior oblique ligament, the meniscus, and the insertions of the semimembranosus tendon. The five insertions of the semimembranosus include the: (1) pars reflexa; (2) direct posteromedial tibial insertion; (3) oblique popliteal ligament insertion; (4) expansion to posterior oblique ligament; and (5) popliteus aponeurosis expansion. (From Sims, WF and Jacobson, KE. The posteromedial corner of the knee: medial-sided injury patterns revisited. Am J Sports Med 2004. 32(2):337-45, permission granted.)

Insertions of the semimembranosus (A), with the numbers (1, 4, 3) corresponding to the Figure 3a legend, are shown in a cadaver. The medial gastrocnemius muscle is cut and elevated proximally (B).
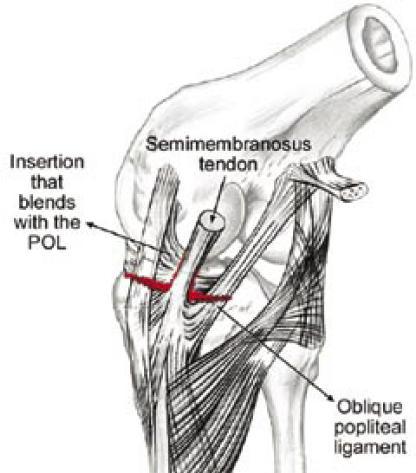
In complete medial-sided knee injuries, the injury completely tears the superficial and deep MCL, as well as the semimembranosus attachments to the femur as shown here. If the knee opens in valgus in extension, usually the posterior oblique and the oblique popliteal ligament extensions from the semimembranosus tendon are ruptured, leaving the semimembranosus attached to the tibia only. These should be repaired at the time of surgery. (Modified from Sims, WF and Jacobson, KE. The posteromedial corner of the knee: medial-sided injury patterns revisited. Am J Sports Med 2004. 32(2):337-45, permission granted.)

A MRI study in an acute injury reveals complete rupture of the superficial and deep MCL from the tibia. The medial meniscus is displaced medially with entrapment of the distal part of the avulsed ligament underneath it (small arrow). Severe hemarthrosis is seen. Please note the bone bruise at the lateral aspect of the lateral femoral condyle suggesting a valgus mechanism (large arrow).

The arthroscopic picture in a case of complete medial-sided knee injury demonstrates pathologic widening of the medial compartment and elevation of the meniscus from the medial tibial articular surface indicating a rupture of the meniscotibial ligament. In this case, the loose fibers of the superficial MCL are seen (arrow). With combined valgus stress and probing, we were able to identify the loose part distally so as to localize the site of the injury. Arthroscopy can also be used in chronic cases to direct the surgeon to the area of laxity below or above the joint.

The intraoperative fluoroscopic picture of a combined ACL reconstruction and a medial-sided knee repair is shown. The two anchors are used to hold the meniscus down to the tibia and the staple is for superficial MCL stabilization.
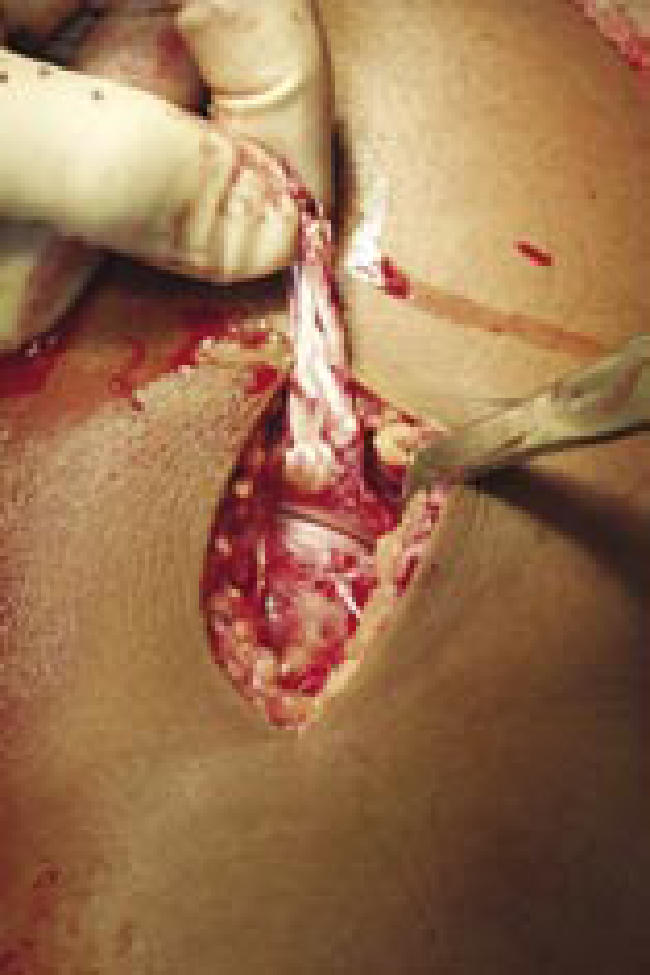
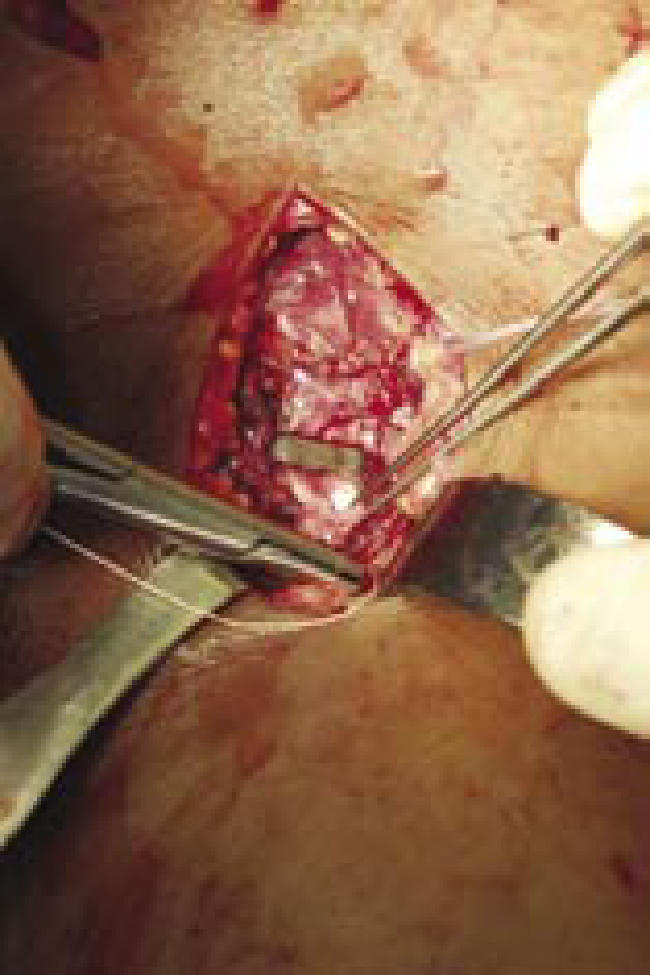
The torn end of the superficial and deep MCL is elevated demonstrating the medial joint space and the medial meniscus.
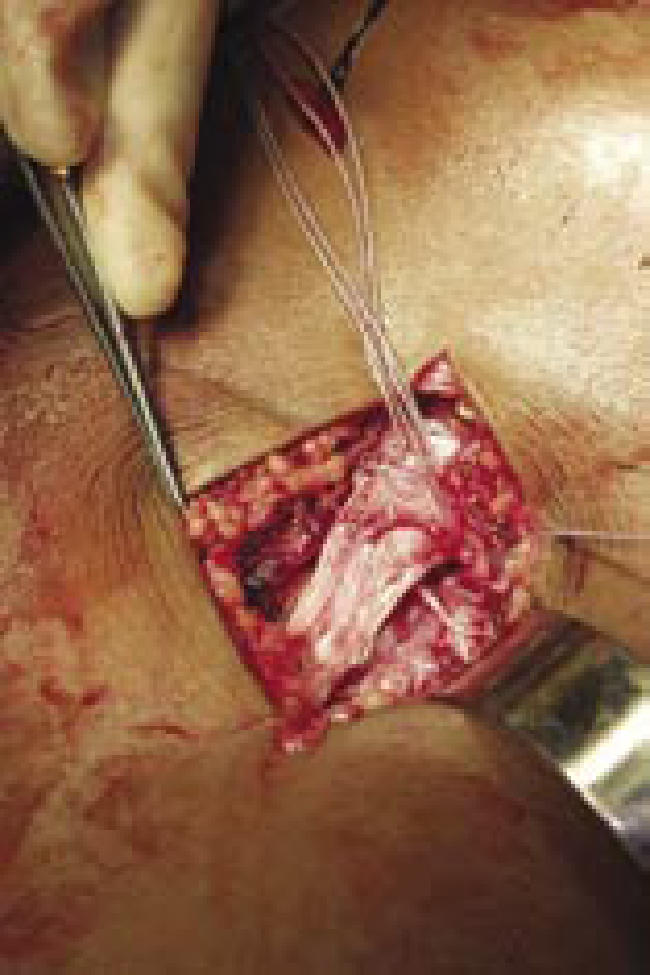
Two anchors were placed and sutures were brought through the peripheral part of the meniscus to repair the deep capsular ligament.
The torn end of the superficial MCL was secured with a staple. The very distal part of the ligament is sutured to the remaining tissue.
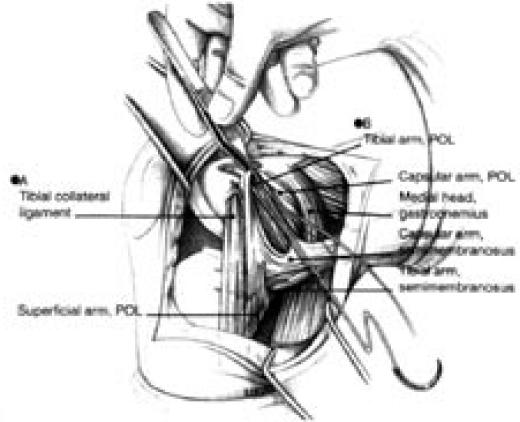
Technique of posteromedial plication demonstrated in a case with proximal avulsion of the superficial MCL and the posterior oblique ligament. Point A demonstrates the location for suture fixation of the superficial MCL to restore tension. With the knee in 60 degrees of flexion and the hip externally rotated, the posterior oblique ligament is pulled anteriorly and proximally to point B where it is being reattached. (From Hughston, JC. The importance of the posterior oblique ligament in repairs of acute tears of the medial ligaments in knees with and without an associated rupture of the ACL. Results of long-term follow-up. J Bone Joint Surg Am 1994. 76(9):1328-44, permission granted.)
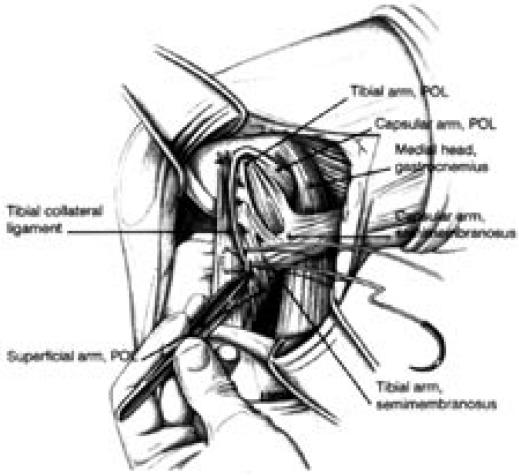
The anterior aspect of the posterior oblique ligament is plicated over the superficial MCL in a pants-over-vest fashion. (From Hughston, JC. The importance of the posterior oblique ligament in repairs of acute tears of the medial ligaments in knees with and without an associated rupture of the ACL. Results of long-term follow-up. J Bone Joint Surg Am 1994. 76(9):1328-44, permission granted.)
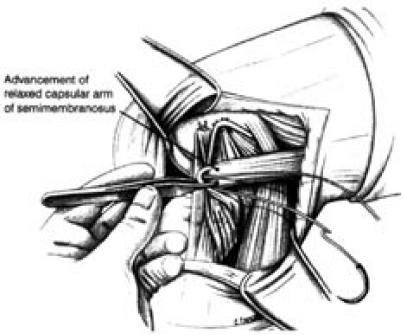
The lax capsular arm of the semimembranosus tendon is plicated over the restored posterior oblique ligament. (From Hughston, JC. The importance of the posterior oblique ligament in repairs of acute tears of the medial ligaments in knees with and without an associated rupture of the ACL. Results of long-term follow- up. J Bone Joint Surg Am 1994. 76(9):1328-44, permission granted.)
References
-
- Fetto JF, Marshall JL. Medial collateral ligament injuries of the knee: a rationale for treatment. Clin Orthop. 1978;132:206–218. - PubMed
-
- Peterson L, et al. Incidence of football injuries and complaints in different age groups and skill-level groups. Am J Sports Med. 2000;28(5 Suppl):S51–S57. - PubMed
-
- Najibi S, Albright JP. The use of knee braces, part 1: Prophylactic knee braces in contact sports. Am J Sports Med. 2005;33(4):602–611. - PubMed
-
- Warme WJ, et al. Ski injury statistics, 1982 to 1993, Jackson Hole Ski Resort. Am J Sports Med. 1995;23(5):597–600. - PubMed
-
- Lorentzon R, Wedren H, Pietila T. Incidence, nature, and causes of ice hockey injuries. A three-year prospective study of a Swedish elite ice hockey team. Am J Sports Med. 1988;16(4):392–396. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical