

Evaluation of Ki-67 proliferation and apoptotic index before, during and after neoadjuvant chemotherapy for primary breast cancer
- PMID: 16790076
- PMCID: PMC1557736
- DOI: 10.1186/bcr1508
Evaluation of Ki-67 proliferation and apoptotic index before, during and after neoadjuvant chemotherapy for primary breast cancer
Abstract
Introduction: Biological markers that reliably predict clinical or pathological response to primary systemic therapy early during a course of chemotherapy may have considerable clinical potential. This study evaluated changes in Ki-67 labeling index and apoptotic index (AI) before, during, and after neoadjuvant anthracycline chemotherapy.
Methods: Twenty-seven patients receiving neoadjuvant FEC (5-fluorouracil, epirubicin, and cyclophosphamide) chemotherapy for operable breast cancer underwent repeat core biopsy after 21 days of treatment. Tissue from pre-treatment biopsy, day 21 and surgery was analysed for Ki-67 index and AI.
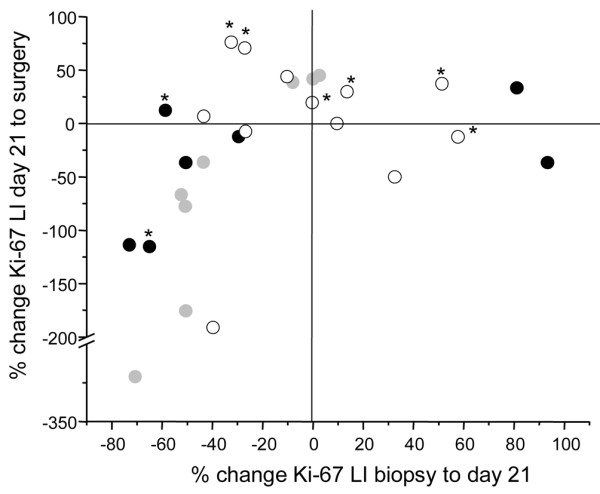
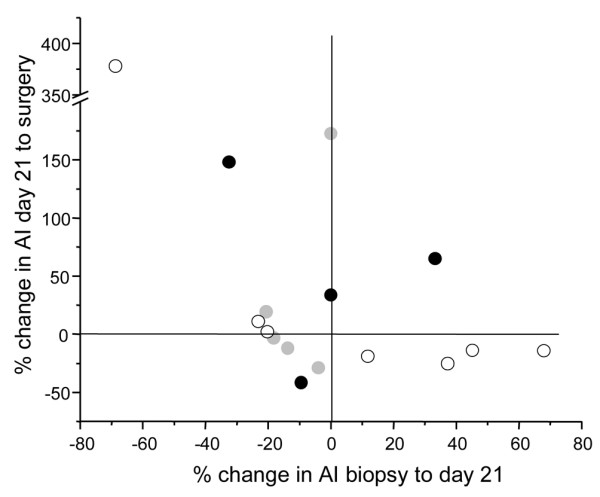
Results: The objective clinical response rate was 56%. Eight patients (31%) achieved a pathological response by histological criteria; two patients had a near-complete pathological response. A reduction in Ki-67 index was observed in 68% of patients at day 21 and 72% at surgery; Ki-67 index increased between day 21 and surgery in 54%. AI decreased in 50% of tumours by day 21, increased in 45% and was unchanged in one patient; 56% demonstrated rebound increases in AI by the time of surgery. Neither pre-treatment nor post-chemotherapy median Ki-67 index nor median AI at all three time points or relative changes at day 21 and surgery differed significantly between clinical or pathological responders and non-responders. Clinical responders had lower median Ki-67 indices at day 21 (11.4% versus 27.0%, p = 0.02) and significantly greater percentage reductions in Ki-67 at day 21 than did non-responders (-50.6% versus -5.3%, p = 0.04). The median day-21 Ki-67 was higher in pathological responders (30.3% versus 14.1%, p = 0.046). A trend toward increased AI at day 21 in pathological responders was observed (5.30 versus 1.68, p = 0.12). Increased day-21 AI was a statistically significant predictor of pathological response (p = 0.049). A strong trend for predicting pathological response was seen with higher Ki-67 indices at day 21 and AI at surgery (p = 0.06 and 0.06, respectively).
Conclusion: The clinical utility of early changes in biological marker expression during chemotherapy remains unclear. Until further prospectively validated evidence confirming the reliability of predictive markers is available, clinical decision-making should not be based upon individual biological tumour marker profiles.
Figures
References
-
- Fisher B, Brown A, Mamounas E, Wieand S, Robidoux A, Margolese RG, Cruz AB, Jr, Fisher ER, Wickerham DL, Wolmark N, et al. Effect of preoperative chemotherapy on local-regional disease in women with operable breast cancer: findings from National Surgical Adjuvant Breast and Bowel Project B-18. J Clin Oncol. 1997;15:2483–2493. - PubMed
-
- Fisher B, Bryant J, Wolmark N, Mamounas E, Brown A, Fisher ER, Wickerham DL, Begovic M, DeCillis A, Robidoux A, et al. Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol. 1998;16:2672–2685. - PubMed
-
- Gasparini G, Boracchi P, Verderio P, Bevilacqua P. Cell kinetics in human breast cancer: comparison between the prognostic value of the cytofluorimetric S-phase fraction and that of the antibodies to Ki-67 and PCNA antigens detected by immunocytochemistry. Int J Cancer. 1994;57:822–829. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
