

How effective are rapid access chest pain clinics? Prognosis of incident angina and non-cardiac chest pain in 8762 consecutive patients
- PMID: 16790531
- PMCID: PMC1861500
- DOI: 10.1136/hrt.2006.090894
How effective are rapid access chest pain clinics? Prognosis of incident angina and non-cardiac chest pain in 8762 consecutive patients
Abstract
Objective: To determine whether rapid access chest pain clinics are clinically effective by comparison of coronary event rates in patients diagnosed with angina with rates in patients diagnosed with non-cardiac chest pain and the general population.
Design: Multicentre cohort study of consecutive patients with chest pain attending the rapid access chest pain clinics (RACPCs) of six hospitals in England.
Participants: 8762 patients diagnosed with either non-cardiac chest pain (n = 6396) or incident angina without prior myocardial infarction (n = 2366) at first cardiological assessment, followed up for a median of 2.57 (interquartile range 1.96-4.15) years.
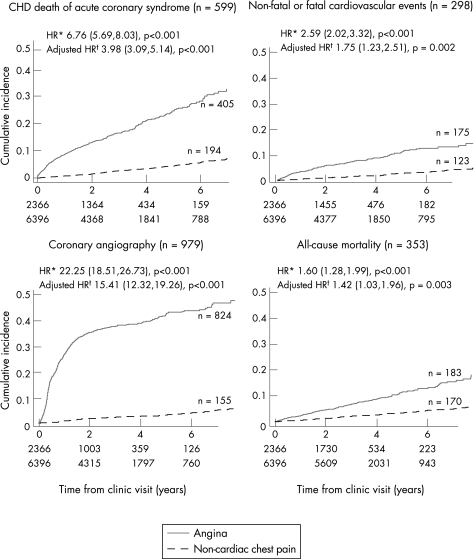
Main outcome measures: Primary end point--death due to coronary heart disease (International Classification of Diseases (ICD)10 I20-I25) or acute coronary syndrome (non-fatal myocardial infarction (ICD10 I21-I23), hospital admission with unstable angina (I24.0, I24.8, I24.9)). Secondary end points--all-cause mortality (ICD I20), cardiovascular death (ICD10 I00-I99), or non-fatal myocardial infarction or non-fatal stroke (I60-I69).
Results: The cumulative probability of the primary end point in patients diagnosed with angina was 16.52% (95% confidence interval (CI) 14.88% to 18.32%) after 3 years compared with 2.73% (95% CI 2.29% to 3.25%) in patients with non-cardiac chest pain. Coronary standardised mortality ratios for men and women with angina aged <65 years were 3.52 (95% CI 1.98 to 5.07) and 4.39 (95% CI 1.14 to 7.64). Of the 599 patients who had the primary end point, 194 (32.4%) had been diagnosed with non-cardiac chest pain. These patients were younger, less likely to have typical symptoms, more likely to be south Asian and more likely to have a normal resting electrocardiogram than patients with angina who had the primary end point.
Conclusion: RACPCs are successful in identifying patients with incident angina who are at high coronary risk, but there is a need to reduce misdiagnosis and improve outcomes in patients diagnosed with non-cardiac chest pain who accounted for nearly one third of cardiac events during follow-up.
Conflict of interest statement
Competing interests: None declared.
Comment in
-
Value of rapid-access chest pain clinics.Heart. 2007 Apr;93(4):415-6. doi: 10.1136/hrt.2006.100248. Heart. 2007. PMID: 17401062 Free PMC article.
References
-
- Kannel W B, Feinleib M. Natural history of angina pectoris in the Framingham study. Prognosis and survival. Am J Cardiol 197229154–163. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical