

Effect of perioperative beta blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial
- PMID: 16793810
- PMCID: PMC1482337
- DOI: 10.1136/bmj.332.7556.1482
Effect of perioperative beta blockade in patients with diabetes undergoing major non-cardiac surgery: randomised placebo controlled, blinded multicentre trial
Abstract
Objectives: To evaluate the long term effects of perioperative beta blockade on mortality and cardiac morbidity in patients with diabetes undergoing major non-cardiac surgery.
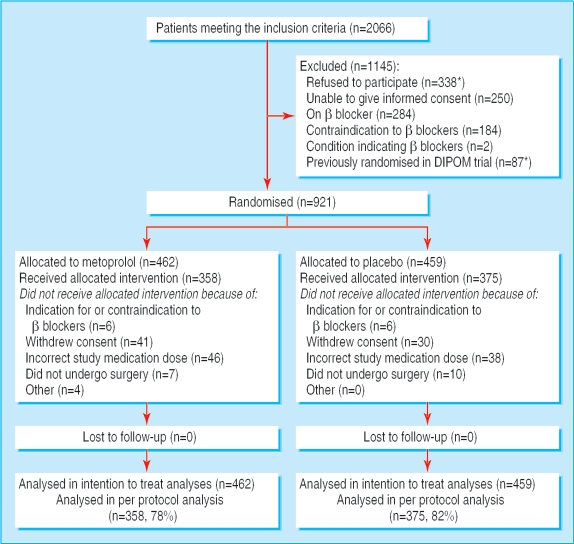
Design: Randomised placebo controlled and blinded multicentre trial. Analyses were by intention to treat.
Setting: University anaesthesia and surgical centres and one coordinating centre.
Participants: 921 patients aged > 39 scheduled for major non-cardiac surgery.
Interventions: 100 mg metoprolol controlled and extended release or placebo administered from the day before surgery to a maximum of eight perioperative days.
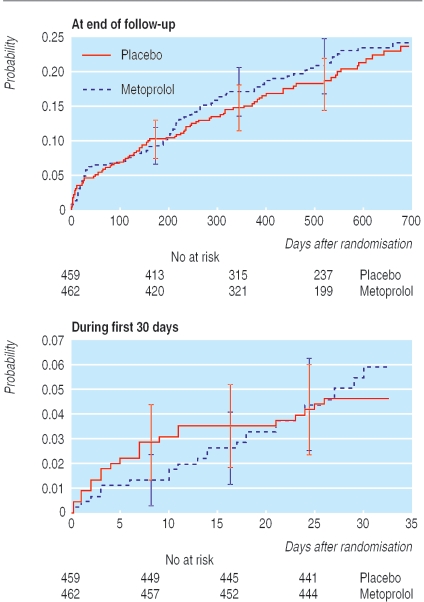
Main outcome measures: The composite primary outcome measure was time to all cause mortality, acute myocardial infarction, unstable angina, or congestive heart failure. Secondary outcome measures were time to all cause mortality, cardiac mortality, and non-fatal cardiac morbidity.
Results: Mean duration of intervention was 4.6 days in the metoprolol group and 4.9 days in the placebo group. Metoprolol significantly reduced the mean heart rate by 11% (95% confidence interval 9% to 13%) and mean blood pressure by 3% (1% to 5%). The primary outcome occurred in 99 of 462 patients in the metoprolol group (21%) and 93 of 459 patients in the placebo group (20%) (hazard ratio 1.06, 0.80 to 1.41) during a median follow-up of 18 months (range 6-30). All cause mortality was 16% (74/462) in the metoprolol group and 16% (72/459) in the placebo group (1.03, 0.74 to 1.42). The difference in risk for the proportion of patients with serious adverse events was 2.4% (- 0.8% to 5.6%).
Conclusions: Perioperative metoprolol did not significantly affect mortality and cardiac morbidity in these patients with diabetes. Confidence intervals, however, were wide, and the issue needs reassessment.
Trial registration: Current Controlled Trials ISRCTN58485613.
Figures
References
-
- Mangano DT, Browner WS, Hollenberg M, Li J, Tateo IM. Long-term cardiac prognosis following noncardiac surgery. The Study of Perioperative Ischemia Research Group. JAMA 1992;268: 233-9. - PubMed
-
- Poldermans D, Boersma E, Bax JJ. The effect of bisoprolol on perioperative mortality and myocardial infarction in high-risk patients undergoing vascular surgery. Dutch Echocardiographic Cardiac Risk Evaluation Applying Stress Echocardiography Study Group. N Engl J Med 1999;341: 1789-94. - PubMed
-
- Ali MJ, Davison P, Pickett W, Ali NS. ACC/AHA guidelines as predictors of postoperative cardiac outcomes. Can J Anaesth 2000;47: 10-9. - PubMed
-
- Goldman L, Caldera DL, Nussbaum SR. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med 1977;297: 845-50. - PubMed
-
- Wallace A, Layug B, Tateo I. Prophylactic atenolol reduces postoperative myocardial ischemia. McSPI Research Group. Anesthesiology 1998;88) :7-17. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical