

Cost-effectiveness of treating multidrug-resistant tuberculosis
- PMID: 16796403
- PMCID: PMC1483913
- DOI: 10.1371/journal.pmed.0030241
Cost-effectiveness of treating multidrug-resistant tuberculosis
Abstract
Background: Despite the existence of effective drug treatments, tuberculosis (TB) causes 2 million deaths annually worldwide. Effective treatment is complicated by multidrug-resistant TB (MDR TB) strains that respond only to second-line drugs. We projected the health benefits and cost-effectiveness of using drug susceptibility testing and second-line drugs in a lower-middle-income setting with high levels of MDR TB.
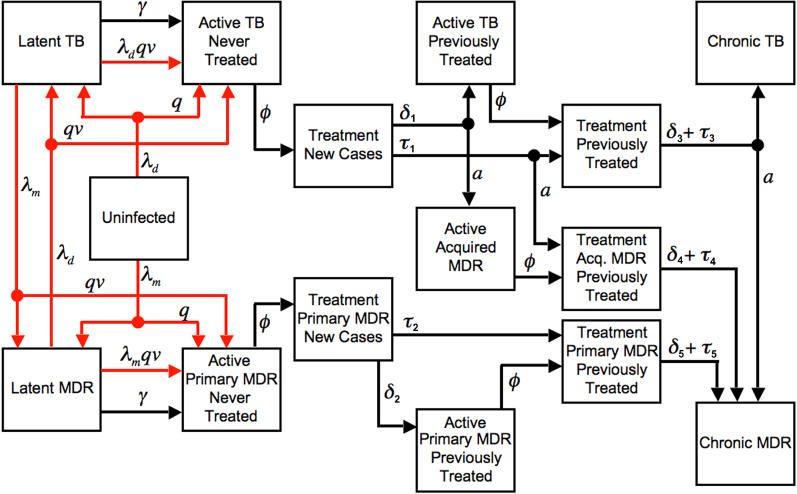
Methods and findings: We developed a dynamic state-transition model of TB. In a base case analysis, the model was calibrated to approximate the TB epidemic in Peru, a setting with a smear-positive TB incidence of 120 per 100,000 and 4.5% MDR TB among prevalent cases. Secondary analyses considered other settings. The following strategies were evaluated: first-line drugs administered under directly observed therapy (DOTS), locally standardized second-line drugs for previously treated cases (STR1), locally standardized second-line drugs for previously treated cases with test-confirmed MDR TB (STR2), comprehensive drug susceptibility testing and individualized treatment for previously treated cases (ITR1), and comprehensive drug susceptibility testing and individualized treatment for all cases (ITR2). Outcomes were costs per TB death averted and costs per quality-adjusted life year (QALY) gained. We found that strategies incorporating the use of second-line drug regimens following first-line treatment failure were highly cost-effective compared to strategies using first-line drugs only. In our base case, standardized second-line treatment for confirmed MDR TB cases (STR2) had an incremental cost-effectiveness ratio of 720 dollars per QALY (8,700 dollars per averted death) compared to DOTS. Individualized second-line drug treatment for MDR TB following first-line failure (ITR1) provided more benefit at an incremental cost of 990 dollars per QALY (12,000 dollars per averted death) compared to STR2. A more aggressive version of the individualized treatment strategy (ITR2), in which both new and previously treated cases are tested for MDR TB, had an incremental cost-effectiveness ratio of 11,000 dollars per QALY (160,000 dollars per averted death) compared to ITR1. The STR2 and ITR1 strategies remained cost-effective under a wide range of alternative assumptions about treatment costs, effectiveness, MDR TB prevalence, and transmission.
Conclusions: Treatment of MDR TB using second-line drugs is highly cost-effective in Peru. In other settings, the attractiveness of strategies using second-line drugs will depend on TB incidence, MDR burden, and the available budget, but simulation results suggest that individualized regimens would be cost-effective in a wide range of situations.
Conflict of interest statement
Figures
Comment in
-
Multidrug-resistant TB in the Philippines: totem and taboo.PLoS Med. 2006 Dec;3(12):e539; author reply e549. doi: 10.1371/journal.pmed.0030539. PLoS Med. 2006. PMID: 17194204 Free PMC article. No abstract available.
-
Cost-effective control of drug-resistant TB: listening to other voices.PLoS Med. 2006 Dec;3(12):e542. doi: 10.1371/journal.pmed.0030542. PLoS Med. 2006. PMID: 17194207 Free PMC article. No abstract available.
References
-
- Dye C, Scheele S, Dolin P, Pathania V, Raviglione MC. Consensus statement. Global burden of tuberculosis: Estimated incidence, prevalence, and mortality by country. WHO Global Surveillance and Monitoring Project. JAMA. 1999;282:677–686. - PubMed
-
- Abdel Aziz M, Wright A, De Muynck A, Laszlo A. Anti-tuberculosis drug resistance in the world: Third global report. Geneva: World Health Organization; 2003. Available: http://whqlibdoc.who.int/publications/2004/9241562854.pdf. Accessed 23 May 2006 .
-
- World Health Organization. Global tuberculosis control: Surveillance, planning, financing—WHO report 2005. Geneva: World Health Organization; 2005. Available: http://www.who.int/tb/publications/global_report/2005/pdf/Full.pdf. Accessed 23 May 2006 .
-
- Murray CJ, DeJonghe E, Chum HJ, Nyangulu DS, Salomao A, et al. Cost effectiveness of chemotherapy for pulmonary tuberculosis in three sub-Saharan African countries. Lancet. 1991;338:1305–1308. - PubMed
-
- China Tuberculosis Control Collaboration. Results of directly observed short-course chemotherapy in 112,842 Chinese patients with smear-positive tuberculosis. Lancet. 1996;347:358–362. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
