

Non ST segment elevation acute coronary syndromes: A simplified risk-orientated algorithm
- PMID: 16801997
- PMCID: PMC2560559
- DOI: 10.1016/s0828-282x(06)70935-7
Non ST segment elevation acute coronary syndromes: A simplified risk-orientated algorithm
Abstract
Non-ST segment elevation acute coronary syndromes (NSTE ACS) include a clinical spectrum that ranges from unstable angina to NSTE myocardial infarction. Management goals aim to prevent recurrent ACS and improve long-term outcomes by choosing a treatment strategy according to an estimate of the risk of an adverse outcome. Recent registry data suggest that patients with NSTE ACS frequently do not receive recommended treatment, and that risk stratification is not used to determine either the choice of treatment or the speed of access to coronary angiography. The present article evaluates the evidence for recommended treatment using information from recent trials and guidelines published by the major cardiac organizations in Europe and North America. Using this information, a multidisciplinary group developed a simplified algorithm that uses risk stratification to select an optimal early management strategy. Long-term outcomes are improved by a multi-faceted vascular protection strategy that is initiated at the time of hospitalization for NSTE ACS.
Les syndromes coronariens aigus sans surélévation du segment ST (SCA SSST) incluent un spectre clinique qui varie de l’angine instable à l’infarctus du myocarde SSST. La prise en charge vise à prévenir une récurrence des SCA et à améliorer les issues à long terme par une stratégie thérapeutique fondée sur une évaluation du risque d’issue négative. D’après les données récentes contenues dans les registres, il n’est pas rare que les patients atteints d’un SCA SSST ne reçoivent pas le traitement recommandé et que la stratification du risque ne soit pas utilisée pour déterminer le choix de traitement ou la vitesse d’accès à une angiographie coronaire.
Le présent article vise à évaluer les données probantes quant aux traitements recommandés au moyen de l’information tirée de récents essais et de récentes lignes directrices publiées par les principaux organismes de cardiologie d’Europe et d’Amérique du Nord. À l’aide de cette information, un groupe multidisciplinaire a mis au point un algorithme simplifié qui fait appel à la stratification du risque pour sélectionner une stratégie optimale de prise en charge précoce. Les issues à long terme s’améliorent grâce à une stratégie de protection vasculaire polyvalente entreprise au moment de l’hospitalisation secondaire à un SCA SSST.
Figures
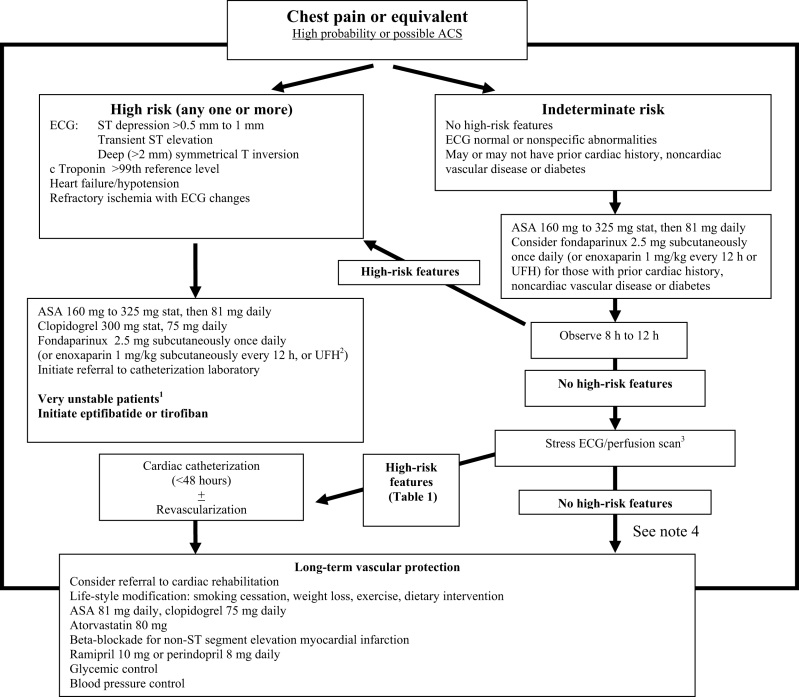
Very unstable patients with one of:
Frequent ischemic episodes with or without pain and electrocardiogram (ECG) ST segment shift;
Very high-risk ECG changes (eg, transient ST elevation or deep ST depression across many leads);
Hemodynamic instability (heart failure or hypotension); or,
Refractory ischemia with ECG ST shift despite acetylsalicylic acid (ASA), clopidogrel and heparin.
Need intensive management with:
Very urgent or immediate cardiac catheterization.
Consider adding intravenous glycoprotein IIb/IIIa inhibitor (tirofiban or eptifibatide) to ASA, clopidogrel and unfractionated heparin (UFH).(if low-molecular-weight heparin has been started, it should be continued and not switched).
Consider use of intra-aortic balloon pump to stabilize the patient before transfer for coronary angiography.
For patients in hospitals where cardiac catheterization will occur within 24 h, UFH should be used.
The stress ECG/perfusion scan ideally should be performed before hospital discharge. This is usually not practical. In patients with a higher probability of more extensive coronary artery disease (prior known coronary disease, multiterritory vascular disease, diabetes and chronic renal insufficiency), short-term admission may be necessary to facilitate early noninvasive testing. In other patients, arrangements should be made for testing in the following few days.
For low-risk patients with a normal stress test, the decision to use long-term vascular protective medication will depend on the patient’s risk factor profile and the clinical history of the acute event. Other causes of chest pain should be considered in many of these patients.
Similar articles
-
Approach to non-ST-segment elevation acute coronary syndrome in the emergency department: risk stratification and treatment strategies.Hosp Pract (1995). 2010 Apr;38(2):40-9. Hosp Pract (1995). 2010. PMID: 20469612
-
Platelet inhibitors in non-ST-segment elevation acute coronary syndromes and percutaneous coronary intervention: glycoprotein IIb/IIIa inhibitors, clopidogrel, or both?Vasc Health Risk Manag. 2006;2(1):39-48. doi: 10.2147/vhrm.2006.2.1.39. Vasc Health Risk Manag. 2006. PMID: 17319468 Free PMC article. Review.
-
Managing acute coronary syndrome: evidence-based approaches.Am J Health Syst Pharm. 2007 Jun 1;64(11 Suppl 7):S14-24. doi: 10.2146/ajhp070109. Am J Health Syst Pharm. 2007. PMID: 17519441
-
Contemporary NSTEMI management: the role of the hospitalist.Hosp Pract (1995). 2020 Feb;48(1):1-11. doi: 10.1080/21548331.2020.1701329. Epub 2020 Feb 20. Hosp Pract (1995). 2020. PMID: 31815570 Review.
-
5-year clinical outcomes in the ICTUS (Invasive versus Conservative Treatment in Unstable coronary Syndromes) trial a randomized comparison of an early invasive versus selective invasive management in patients with non-ST-segment elevation acute coronary syndrome.J Am Coll Cardiol. 2010 Mar 2;55(9):858-64. doi: 10.1016/j.jacc.2009.11.026. Epub 2010 Jan 4. J Am Coll Cardiol. 2010. PMID: 20045278 Clinical Trial.
Cited by
-
Risk stratification and in-hospital outcome in patients with acute coronary syndrome.J Family Med Prim Care. 2022 Jun;11(6):2780-2788. doi: 10.4103/jfmpc.jfmpc_1805_21. Epub 2022 Jun 30. J Family Med Prim Care. 2022. PMID: 36119317 Free PMC article.
-
Pattern and Outcome of Acute Non-ST-Segment Elevation Myocardial Infarction Seen in Adult Emergency Department of Al-Shaab Teaching Hospital: A prospective Observational Study in a Tertiary Cardiology Center.Cureus. 2021 Sep 14;13(9):e17981. doi: 10.7759/cureus.17981. eCollection 2021 Sep. Cureus. 2021. PMID: 34540510 Free PMC article.
-
The impact of bleeding in patients with acute coronary syndromes: how to optimize the benefits of treatment and minimize the risk.Can J Cardiol. 2007 Jun;23(8):663-71. doi: 10.1016/s0828-282x(07)70229-5. Can J Cardiol. 2007. PMID: 17593993 Free PMC article. Review.
-
Prognostic Value of the RISK-PCI Score in Patients with Non-ST-Segment Elevation Acute Myocardial Infarction.J Clin Med. 2025 Apr 16;14(8):2727. doi: 10.3390/jcm14082727. J Clin Med. 2025. PMID: 40283557 Free PMC article.
References
-
- Davies MJ. The contribution of thrombosis to the clinical expression of coronary atherosclerosis. Thromb Res. 1996;82:1–32. - PubMed
-
- Davies MJ. Stability and instability: Two faces of coronary atherosclerosis. The Paul Dudley White Lecture 1995. Circulation. 1996;94:2013–20. - PubMed
-
- DeWood MA, Stifter WF, Simpson CS, et al. Coronary arteriographic findings soon after non-Q-wave myocardial infarction. N Engl J Med. 1986;315:417–23. - PubMed
-
- Savonitto S, Ardissino D, Granger CB, et al. Prognostic value of the admission electrocardiogram in acute coronary syndromes. JAMA. 1999;281:707–13. - PubMed
-
- Fitchett DH University of Toronto Division of Cardiology and the Greater Toronto Area Community Cardiologists. Guidelines for the early management of acute coronary syndromes. Can J Cardiol. 2000;16:1423–32. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
