

Sphincter of Oddi dysfunction: managing the patient with chronic biliary pain
- PMID: 16804961
- PMCID: PMC4087924
- DOI: 10.3748/wjg.v12.i24.3793
Sphincter of Oddi dysfunction: managing the patient with chronic biliary pain
Abstract
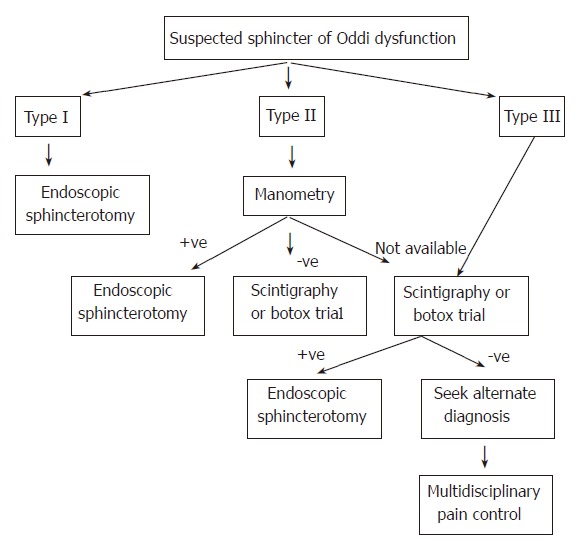
Sphincter of Oddi dysfunction (SOD) is a syndrome of chronic biliary pain or recurrent pancreatitis due to functional obstruction of pancreaticobiliary flow at the level of the sphincter of Oddi. The Milwaukee classification stratifies patients according to their clinical picture based on elevated liver enzymes, dilated common bile duct and presence of abdominal pain. Type I patients have pain as well as abnormal liver enzymes and a dilated common bile duct. Type II SOD consists of pain and only one objective finding, and Type III consists of biliary pain only. This classification is useful to guide diagnosis and management of sphincter of Oddi dysfunction. The current gold standard for diagnosis is manometry to detect elevated sphincter pressure, which correlates with outcome to sphincterotomy. However, manometry is not widely available and is an invasive procedure with a risk of pancreatitis. Non-invasive testing methods, including fatty meal ultrasonography and scintigraphy, have shown limited correlation with manometric findings but may be useful in predicting outcome to sphincterotomy. Endoscopic injection of botulinum toxin appears to predict subsequent outcome to sphincterotomy, and could be useful in selection of patients for therapy, especially in the setting where manometry is unavailable.
Figures
References
-
- Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Thompson WG, Whitehead WE, Janssens J, Funch-Jensen P, Corazziari E. U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci. 1993;38:1569–1580. - PubMed
-
- Bar-Meir S, Halpern Z, Bardan E, Gilat T. Frequency of papillary dysfunction among cholecystectomized patients. Hepatology. 1984;4:328–330. - PubMed
-
- Meshkinpour H, Mollot M. Sphincter of Oddi dysfunction and unexplained abdominal pain: clinical and manometric study. Dig Dis Sci. 1992;37:257–261. - PubMed
-
- Meshkinpour H, Mallot M. Bile duct dyskinesia and unexplained abdominal pain: A clinical and manometric study. Gastroenterology. 1987;92:1533A. - PubMed
-
- Venu RP, Geenen JE, Hogan W, Stone J, Johnson GK, Soergel K. Idiopathic recurrent pancreatitis. An approach to diagnosis and treatment. Dig Dis Sci. 1989;34:56–60. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
