

A population study of the long-term consequences of Rose angina: 20-year follow-up of the Renfrew-Paisley study
- PMID: 16807274
- PMCID: PMC1861298
- DOI: 10.1136/hrt.2006.090118
A population study of the long-term consequences of Rose angina: 20-year follow-up of the Renfrew-Paisley study
Abstract
Objective: To examine the long-term cardiovascular consequences of angina in a large epidemiological study.
Design: Prospective cohort study conducted between 1972 and 1976 with 20 years of follow-up (the Renfrew-Paisley Study).
Setting: Renfrew and Paisley, West Scotland, UK.
Participants: 7048 men and 8354 women aged 45-64 years who underwent comprehensive cardiovascular screening at baseline, including the Rose Angina Questionnaire and electrocardiography (ECG).
Main outcome measures: All deaths and hospitalisations for cardiovascular reasons occurring over the subsequent 20 years, according to the baseline Rose angina score and baseline ECG.
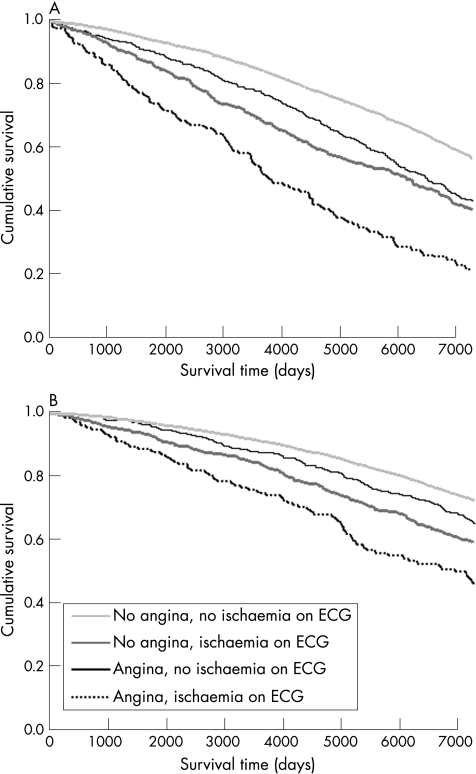
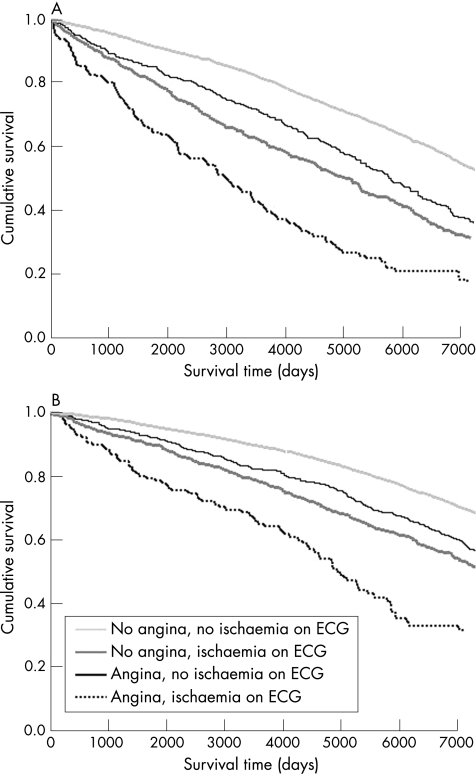
Results: At baseline, 669 (9.5%) men and 799 (9.6%) women had angina on Rose Angina Questionnaire. All-cause mortality for those with Rose angina was 67.7% in men and 43.3% in women at 20 years compared with 45.4% and 30.4%, respectively, in those without angina (p<0.001). Values are expressed as hazards ratio (HR) (95% confidence interval (CI). In a multivariate analysis, men with Rose angina had an increased risk of cardiovascular death or hospitalisation (1.49 (1.33 to 1.66), myocardial infarction (1.63 (1.41 to 1.85)) or heart failure (1.54 (1.13 to 2.10)) compared with men without angina. The corresponding HR (95% CI) for women were 1.38 (1.23 to 1.55), 1.56 (1.31 to 1.85) and 1.92 (1.44 to 2.56). An abnormality on the electrocardiogram (ECG) increased risk further, and both angina and an abnormality on the ECG increased risk most of all compared with those with neither angina nor ischaemic changes on the ECG. Compared with men, women with Rose angina were less likely to have a cardiovascular event (0.54 (0.46 to 0.64)) or myocardial infarction (0.44 (0.35 to 0.56)), although there was no sex difference in the risk of stroke (1.11 (0.75 to 1.65)), atrial fibrillation (0.84 (0.38 to 1.87)) or heart failure (0.79 (0.51 to 1.21)).
Conclusions: Angina in middle age substantially increases the risk of death, myocardial infarction, heart failure and other cardiovascular events.
Conflict of interest statement
Competing interests: None.
References
-
- Kannel W B, Feinleib M. Natural history of angina pectoris in the Framingham Study. Prognosis and survival. Am J Cardiol 197229154–163. - PubMed
-
- Orencia A, Bailey K, Yawn B P.et al Effect of gender on long‐term outcome of angina pectoris and myocardial infarction/sudden unexpected death. JAMA 19932692392–2397. - PubMed
-
- Murabito J M, Evans J C, Larson M G.et al Prognosis after the onset of coronary heart disease. An investigation of differences in outcome between the sexes according to initial coronary disease presentation. Circulation 1993882548–2555. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical