

Bilateral facial paralysis: case presentation and discussion of differential diagnosis
- PMID: 16808763
- PMCID: PMC1924702
- DOI: 10.1111/j.1525-1497.2006.00466.x
Bilateral facial paralysis: case presentation and discussion of differential diagnosis
Abstract
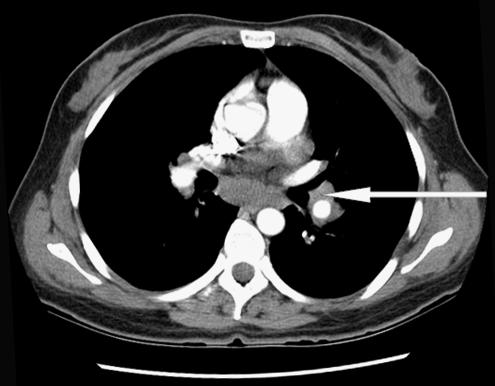
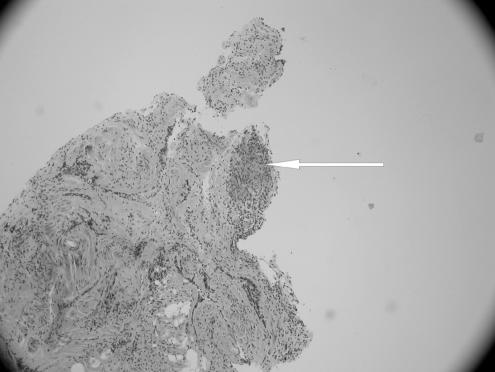
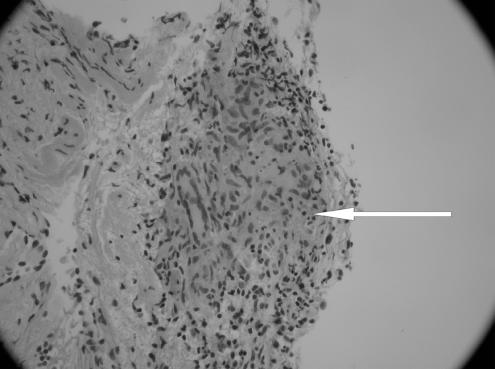
Bilateral facial paralysis is a rare condition and therefore represents a diagnostic challenge. We report the case of a 34-year-old healthy woman with sequential bilateral facial paralysis as a sole manifestation of sarcoidosis. She initially presented with an isolated left sided Bell's palsy without any symptoms to suggest alternative diagnoses. Within a month there was progression to peripheral facial paresis on the contra lateral side, prompting a diagnosis of Lyme disease. Her physical examination and chest x-ray did not reveal any clinical evidence of sarcoidosis. After failing to respond to an empiric trial of intravenous ceftriaxone for a presumptive diagnosis of Lyme disease, computed tomography scan of the chest was ordered which demonstrated bilateral hilar lymphadenopathy. Bronchoscopic biopsy confirmed a diagnosis of sarcoidosis. The patient then made a complete recovery on steroid therapy. We discuss the differential diagnosis of facial diplegia and focus on the clinical presentation, diagnosis and treatment of neurosarcoidosis.
Figures
References
-
- Adour KK, Byl FM, Hilsinger RL, Kahn ZM, Sheldon MI. The true nature of Bell's palsy: analysis of 1,000 consecutive patients. Laryngoscope. 1978;88:787–801. - PubMed
-
- Stahl N, Ferit T. Recurrent bilateral peripheral facial palsy. J Laryngol Otol. 1989;103:117–9. - PubMed
-
- McIntosh WE, Brenner JF, Aschenbrenner JE. Bilateral facial paralysis as the sole presenting feature of sarcoidosis: report of a case. J Am Osteopath Assoc. 1987;87:245–7. - PubMed
-
- George MK, Pahor AL. Sarcoidosis: a cause for bilateral facial palsy. Ear Nose Throat J. 1991;70:492–3. - PubMed
-
- Haydar A, Hujairi NM, Tawil A. Bilateral facial paralysis: what's the cause? Med J Am. 2003;179:553. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources