

Primary care clinicians treat patients with medically unexplained symptoms: a randomized controlled trial
- PMID: 16808764
- PMCID: PMC1924714
- DOI: 10.1111/j.1525-1497.2006.00460.x
Primary care clinicians treat patients with medically unexplained symptoms: a randomized controlled trial
Abstract
Objective: There is no proven primary care treatment for patients with medically unexplained symptoms (MUS). We hypothesized that a long-term, multidimensional intervention by primary care providers would improve MUS patients' mental health.
Design: Clinical trial.
Setting: HMO in Lansing, MI.
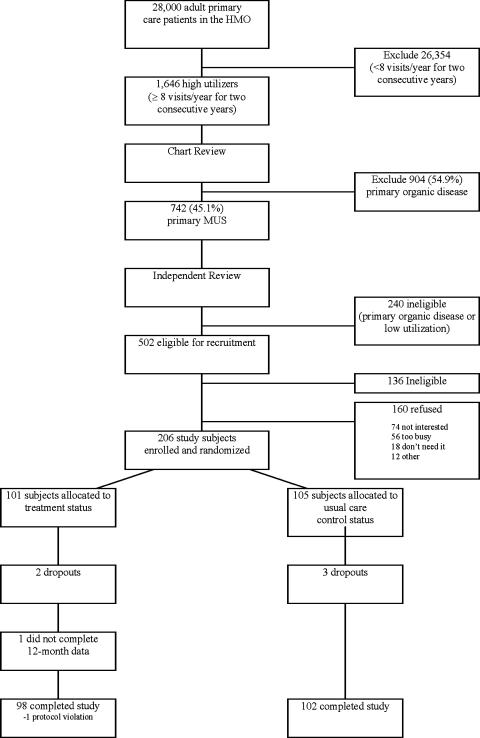
Participants: Patients from 18 to 65 years old with 2 consecutive years of high utilization were identified as having MUS by a reliable chart rating procedure; 206 subjects were randomized and 200 completed the study.
Intervention: From May 2000 to January 2003, 4 primary care clinicians deployed a 12-month intervention consisting of cognitive-behavioral, pharmacological, and other treatment modalities. A behaviorally defined patient-centered method was used by clinicians to facilitate this treatment and the provider-patient relationship.
Main outcome measure: The primary endpoint was an improvement from baseline to 12 months of 4 or more points on the Mental Component Summary of the SF-36.
Results: Two hundred patients averaged 13.6 visits for the year preceding study. The average age was 47.7 years and 79.1% were females. Using intent to treat, 48 treatment and 34 control patients improved (odds ratio [OR]=1.92, 95% confidence interval [CI]: 1.08 to 3.40; P=.02). The relative benefit (relative "risk" for improving) was 1.47 (CI: 1.05 to 2.07), and the number needed to treat was 6.4 (95% CI: 0.89 to 11.89). The following baseline measures predicted improvement: severe mental dysfunction (P<.001), severe body pain (P=.039), nonsevere physical dysfunction (P=.003), and at least 16 years of education (P=.022); c-statistic=0.75.
Conclusion: The first multidimensional intervention by primary care clinicians led to clinically significant improvement in MUS patients.
Figures
References
-
- deGruy F, Columbia L, Dickinson P. Somatization disorder in a family practice. J Fam Pract. 1987;25:45–51. - PubMed
-
- 4. Washington, DC: American Psychiatric Association; 1994. American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders.
-
- Escobar JI, Waitzkin H, Silver RC, Gara M, Holman A. Abridged somatization: a study in primary care. Psychosom Med. 1998;60:466–72. - PubMed
-
- Bridges KW, Goldberg DP. Somatic presentation of DSM III psychiatric disorders in primary care. J Psychosom Res. 1985;29:563–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical