

Inequalities in health: a comparative study between ethnic Norwegians and Pakistanis in Oslo, Norway
- PMID: 16808838
- PMCID: PMC1553452
- DOI: 10.1186/1475-9276-5-7
Inequalities in health: a comparative study between ethnic Norwegians and Pakistanis in Oslo, Norway
Abstract
Background: The objective of the study was to observe the inequality in health from the perspective of socio-economic factors in relation to ethnic Pakistanis and ethnic Norwegians in Oslo, Norway.
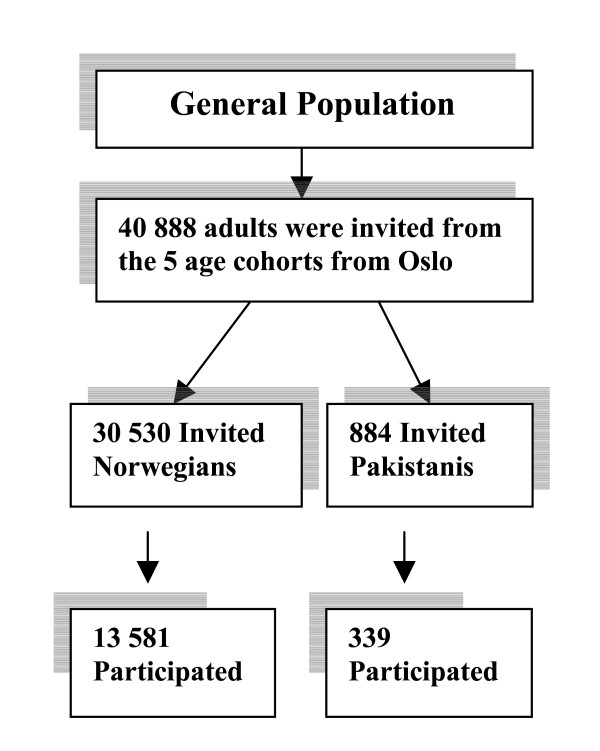
Method: Data was collected by using an open and structured questionnaire, as a part of the Oslo Health Study 2000-2001. Accordingly 13581 ethnic Norwegians (45% of the eligible) participated as against 339 ethnic Pakistanis (38% of the eligible).
Results: The ethnic Pakistanis reported a higher prevalence of poor self-rated health 54.7% as opposed to 22.1% (p < 0.001) in ethnic Norwegians, 14% vs. 2.6% (p < 0.001) in diabetes, and 22.0% vs. 9.9% (p < 0.001) in psychological distress. The socio-economic conditions were inversely related to self-rated health, diabetes and distress for the ethnic Norwegians. However, this was surprisingly not the case for the ethnic Pakistanis. Odd ratios did not interfere with the occurrence of diabetes, even after adjusting all the markers of socio-economic status in the multivariate model, while self-reported health and distress showed moderate reduction in the risk estimation.
Conclusion: There is a large diversity of self-rated health, prevalence of diabetes and distress among the ethnic Pakistanis and Norwegians. Socio-economic status may partly explain the observed inequalities in health. Uncontrolled variables like genetics, lifestyle factors and psychosocial factors related to migration such as social support, community participation, discrimination, and integration may have contributed to the observed phenomenon. This may underline the importance of a multidisciplinary approach in future studies.
Similar articles
-
Psychosocial factors and distress: a comparison between ethnic Norwegians and ethnic Pakistanis in Oslo, Norway.BMC Public Health. 2006 Jul 10;6:182. doi: 10.1186/1471-2458-6-182. BMC Public Health. 2006. PMID: 16831229 Free PMC article.
-
Pakistanis living in Oslo have lower serum 1,25-dihydroxyvitamin D levels but higher serum ionized calcium levels compared with ethnic Norwegians. The Oslo Health Study.BMC Endocr Disord. 2007 Oct 18;7:9. doi: 10.1186/1472-6823-7-9. BMC Endocr Disord. 2007. PMID: 17945003 Free PMC article.
-
Biochemical markers of bone turnover and their relation to forearm bone mineral density in persons of Pakistani and Norwegian background living in Oslo, Norway: The Oslo Health Study.Eur J Endocrinol. 2006 Nov;155(5):693-9. doi: 10.1530/eje.1.02282. Eur J Endocrinol. 2006. PMID: 17062885
-
Cardiovascular disease by diabetes status in five ethnic minority groups compared to ethnic Norwegians.BMC Public Health. 2011 Jul 13;11:554. doi: 10.1186/1471-2458-11-554. BMC Public Health. 2011. PMID: 21752237 Free PMC article.
-
Assessing social differences in overweight among 15- to 16-year-old ethnic Norwegians from Oslo by register data and adolescent self-reported measures of socio-economic status.Int J Obes (Lond). 2007 Jan;31(1):30-8. doi: 10.1038/sj.ijo.0803415. Epub 2006 Jun 20. Int J Obes (Lond). 2007. PMID: 16788570
Cited by
-
Immigration, social integration and mental health in Norway, with focus on gender differences.Clin Pract Epidemiol Ment Health. 2007 Oct 30;3:24. doi: 10.1186/1745-0179-3-24. Clin Pract Epidemiol Ment Health. 2007. PMID: 17971211 Free PMC article.
-
Psychosocial factors and distress: a comparison between ethnic Norwegians and ethnic Pakistanis in Oslo, Norway.BMC Public Health. 2006 Jul 10;6:182. doi: 10.1186/1471-2458-6-182. BMC Public Health. 2006. PMID: 16831229 Free PMC article.
-
Health status sensed by the adult Latin American immigrant population in the city of Seville, Spain.J Immigr Minor Health. 2015 Jun;17(3):820-5. doi: 10.1007/s10903-013-9963-9. J Immigr Minor Health. 2015. PMID: 24346840
-
Antidepressant utilization after hospitalization with depression: a comparison between non-Western immigrants and Danish-born residents.BMC Psychiatry. 2014 Mar 17;14:77. doi: 10.1186/1471-244X-14-77. BMC Psychiatry. 2014. PMID: 24636339 Free PMC article.
-
Health-Related Quality of Life, Subjective Health Complaints, Psychological Distress and Coping in Pakistani Immigrant Women With and Without the Metabolic Syndrome : The InnvaDiab-DEPLAN Study on Pakistani Immigrant Women Living in Oslo, Norway.J Immigr Minor Health. 2011 Aug;13(4):732-41. doi: 10.1007/s10903-010-9409-6. J Immigr Minor Health. 2011. PMID: 21061066 Free PMC article.
References
-
- Acheson D. Independent inquiry into inequalities in health. London, TSO; 1998.
-
- Davey Smith G, Blane D, Bartley M. Explanations for socioeconomic differentials in mortality: evidence from Britain and elsewhere. European Journal of Public Health. 1994. pp. 131–144.
-
- Leon D, Walt G. poverty, inequality and health: an international perspective. Oxford: Oxford University Press; 2001.
-
- Strickland S, Shetty P. Human biology and social inequality. Cambridge: Cambridge University Press; 1998.
LinkOut - more resources
Full Text Sources
