

Modifications of coronary risk factors
- PMID: 16813737
- PMCID: PMC2670550
- DOI: 10.1016/j.amjcard.2006.03.012
Modifications of coronary risk factors
Abstract
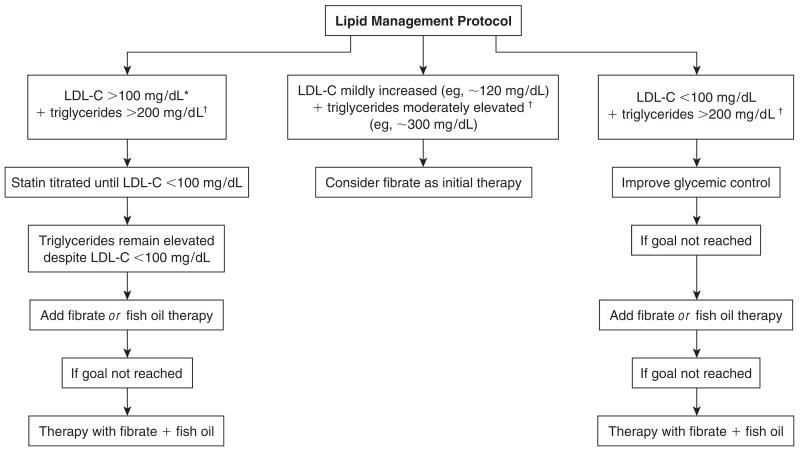
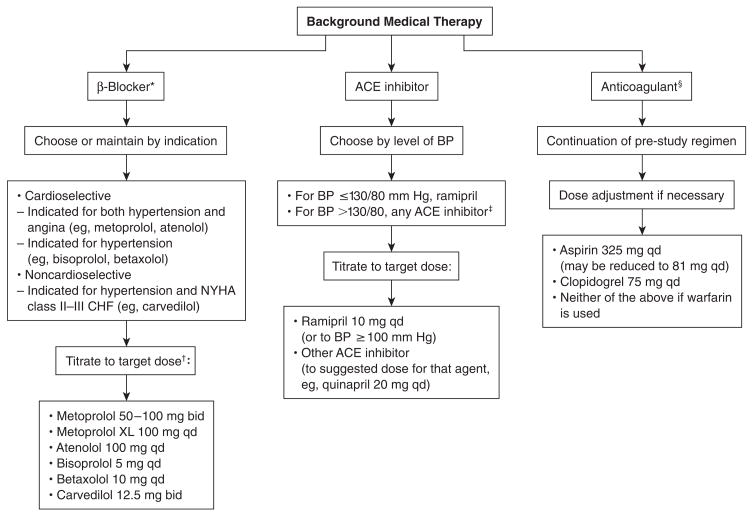
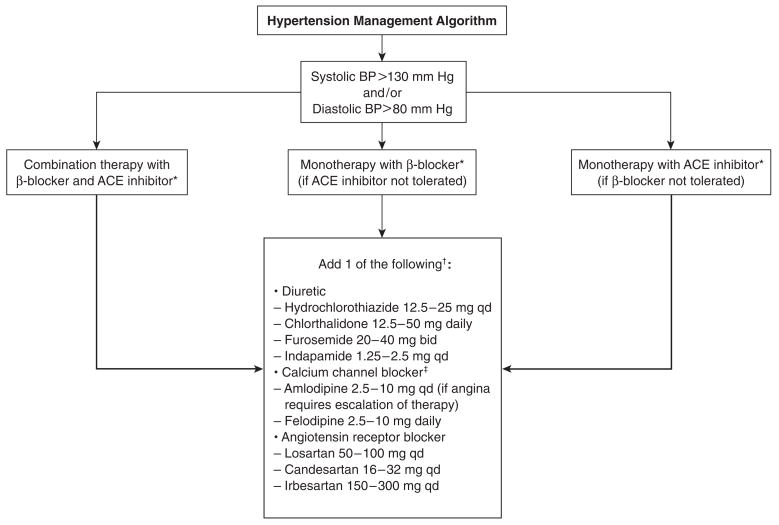
In addition to the revascularization and glycemic management interventions assigned at random, the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI 2D) design includes the uniform control of major coronary artery disease risk factors, including dyslipidemia, hypertension, smoking, central obesity, and sedentary lifestyle. Target levels for risk factors were adjusted throughout the trial to comply with changes in recommended clinical practice guidelines. At present, the goals are low-density lipoprotein cholesterol <2.59 mmol/L (<100 mg/dL) with an optional goal of <1.81 mmol/L (<70 mg/dL); plasma triglyceride level <1.70 mmol/L (<150 mg/dL); blood pressure level <130 mm Hg systolic and <80 mm Hg diastolic; and smoking cessation treatment for all active smokers. Algorithms were developed for the pharmacologic management of dyslipidemia and hypertension. Dietary prescriptions for the management of glycemia, plasma lipid profiles, and blood pressure levels were adapted from existing clinical practice guidelines. Patients with a body mass index >25 were prescribed moderate caloric restriction; after the trial was under way, a lifestyle weight-management program was instituted. All patients were formally prescribed both endurance and resistance/flexibility exercises, individually adapted to their level of disability and fitness. Pedometers were distributed as a biofeedback strategy. Strategies to achieve the goals for risk factors were designed by BARI 2D working groups (lipid, cardiovascular and hypertension, and nonpharmacologic intervention) and the ongoing implementation of the strategies is monitored by lipid, hypertension, and lifestyle intervention management centers.
Figures
References
-
- American Diabetes Association. American Diabetes Association Consensus Statement: Role of cardiovascular risk factors in prevention and treatment of macrovascular disease in diabetes. Diabetes Care. 1989;12:573–579. - PubMed
-
- Turner RC, Millns H, Neil HAW, Stratton IM, Manley SE, Matthews DR, Holman RR for the United Kingdom Prospective Diabetes Study Group. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS: 23) BMJ. 1998;316:823–828. - PMC - PubMed
-
- Suarez L, Barrett-Connor E. Interaction between cigarette smoking and diabetes mellitus in the prediction of death attributed to cardiovascular disease. Am J Epidemiol. 1984;120:670–675. - PubMed
-
- Haire-Joshu D, Glasgow RE, Tibbs TL. Smoking and diabetes. Diabetes Care. 1999;22:1887–1898. - PubMed
-
- Eliasson B. Cigarette smoking and diabetes. Prog Cardiovasc Dis. 2003;45:405–413. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
