

Continuing controversy over monitoring men with localized prostate cancer: a systematic review of programs in the prostate specific antigen era
- PMID: 16813862
- PMCID: PMC2875171
- DOI: 10.1016/j.juro.2006.03.030
Continuing controversy over monitoring men with localized prostate cancer: a systematic review of programs in the prostate specific antigen era
Abstract
Purpose: There is continuing controversy over the most appropriate treatment for screen detected and clinically localized prostate cancer, and increasing interest in monitoring such men initially with radical treatment targeted at cancers showing signs of progressive potential but while they are still curable. Current evidence on monitoring protocols and biomarkers used to predict disease progression was systematically reviewed.
Materials and methods: The MEDLINE and Excerpta Medica (EMBASE) bibliographic databases were searched from 1988 to October 2004, supplemented by manual searches of reference lists, focusing on studies reporting monitoring of men with localized prostate cancer.
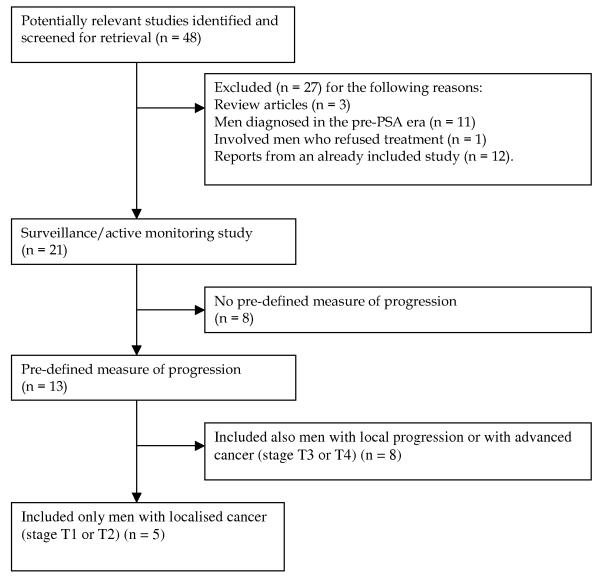
Results: A total of 48 potentially eligible articles were found but only 5 studies, in which there was a total of 451 participants, restricted entry criteria to men with clinically localized (T1-T2) prostate cancer. Monitoring protocols varied with little consensus, although the majority used prostate specific antigen and digital rectal examination, while some added re-biopsy to assess progression. Actuarial probabilities of freedom from disease progression at 4 to 5 years of followup were 67% to 72%. However, up to 50% of men abandoned monitoring within 2 years, largely because of anxiety related to increasing prostate specific antigen rather than objective evidence of disease progression. There was no robust evidence to support prostate specific antigen doubling times or velocity to identify men in whom disease may progress. Studies were characterized by small sample size, short-term followup, observer bias and uncertain validity around variable definitions of progression.
Conclusions: Current evidence suggests that some form of monitoring would be a suitable treatment option in men with localized prostate cancer but there is little consensus over what markers should be used in such a program or how progression should be properly defined. The search for a method that safely identifies men with prostate cancer who could avoid radical intervention must continue.
Figures
Similar articles
-
Home treatment for mental health problems: a systematic review.Health Technol Assess. 2001;5(15):1-139. doi: 10.3310/hta5150. Health Technol Assess. 2001. PMID: 11532236
-
Eliciting adverse effects data from participants in clinical trials.Cochrane Database Syst Rev. 2018 Jan 16;1(1):MR000039. doi: 10.1002/14651858.MR000039.pub2. Cochrane Database Syst Rev. 2018. PMID: 29372930 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Early versus deferred androgen suppression in the treatment of advanced prostatic cancer.Cochrane Database Syst Rev. 2002;(1):CD003506. doi: 10.1002/14651858.CD003506. Cochrane Database Syst Rev. 2002. Update in: Cochrane Database Syst Rev. 2019 Jun 11;6:CD003506. doi: 10.1002/14651858.CD003506.pub2. PMID: 11869665 Updated.
-
The measurement and monitoring of surgical adverse events.Health Technol Assess. 2001;5(22):1-194. doi: 10.3310/hta5220. Health Technol Assess. 2001. PMID: 11532239
Cited by
-
Active surveillance for low-risk prostate cancer: diversity of practice across Europe.Ir J Med Sci. 2015 Jun;184(2):305-11. doi: 10.1007/s11845-014-1104-5. Epub 2014 Mar 21. Ir J Med Sci. 2015. PMID: 24652265
-
Factors influencing patients' acceptance and adherence to active surveillance.J Natl Cancer Inst Monogr. 2012 Dec;2012(45):207-12. doi: 10.1093/jncimonographs/lgs024. J Natl Cancer Inst Monogr. 2012. PMID: 23271775 Free PMC article.
-
Active surveillance or active treatment in localized prostate cancer?Dtsch Arztebl Int. 2009 May;106(22):371-6. doi: 10.3238/arztebl.2009.0371. Epub 2009 May 29. Dtsch Arztebl Int. 2009. PMID: 19623304 Free PMC article. Review.
-
Communicating risk in active surveillance of localised prostate cancer: a protocol for a qualitative study.BMJ Open. 2017 Oct 5;7(10):e017372. doi: 10.1136/bmjopen-2017-017372. BMJ Open. 2017. PMID: 28982830 Free PMC article.
-
Current strategies for monitoring men with localised prostate cancer lack a strong evidence base: observational longitudinal study.Br J Cancer. 2009 Aug 4;101(3):390-4. doi: 10.1038/sj.bjc.6605181. Epub 2009 Jul 14. Br J Cancer. 2009. PMID: 19603015 Free PMC article.
References
-
- Parkin DM, Bray FI, Devesa SS. Cancer burden in the year 2000. The global picture. European Journal of Cancer. 2001;37(Supplement 8):4–66. - PubMed
-
- Whitmore WF. Localised prostatic cancer: management and detection issues. Lancet. 1994;343(8908):1263–7. - PubMed
-
- Eisenberger M, Partin A. Progress toward Identifying Aggressive Prostate Cancer. N Engl J Med. 2004;351(2):180–1. - PubMed
-
- Frankel S, Smith GD, Donovan J, Neal D. Screening for prostate cancer. Lancet. 2003;361(9363):1122–8. - PubMed
-
- Gerber GS, Gornik HL, Goldfischer ER, Chodak GW, Rukstalis DB. Evaluation of changes in prostate specific antigen in clinically localized prostate cancer managed without initial therapy. Journal of Urology. 1998;159(4):1243–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
