

The relationship between somatic growth and in vivo esophageal segmental and sphincteric growth in human neonates
- PMID: 16819375
- PMCID: PMC4028631
- DOI: 10.1097/01.mpg.0000226368.24332.50
The relationship between somatic growth and in vivo esophageal segmental and sphincteric growth in human neonates
Abstract
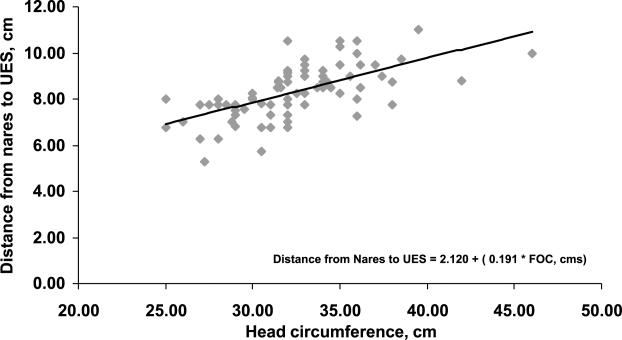
Background: Measurement of aerodigestive tract length is an important determinant for accurate placement of esophageal probes and gavage tubes at the desired location. The relationship of esophageal body, upper esophageal sphincter (UES) and lower esophageal sphincter (LES) lengths with somatic growth in neonates is not well understood.
Objectives: Our objectives were to (1) evaluate a relationship between segmental esophageal lengths and somatic growth parameters and (2) ascertain the relationship between segmental esophageal lengths and gestational age (GA) and postmenstrual age (PMA) in preterm and full-term born human neonates.
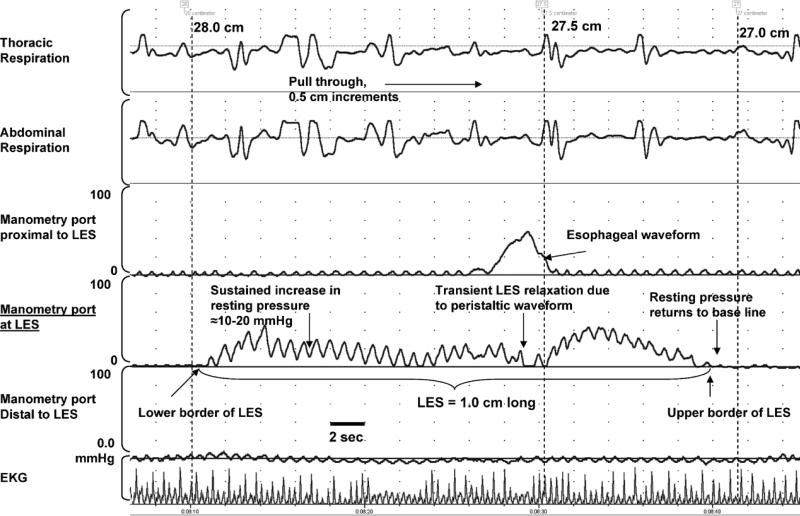
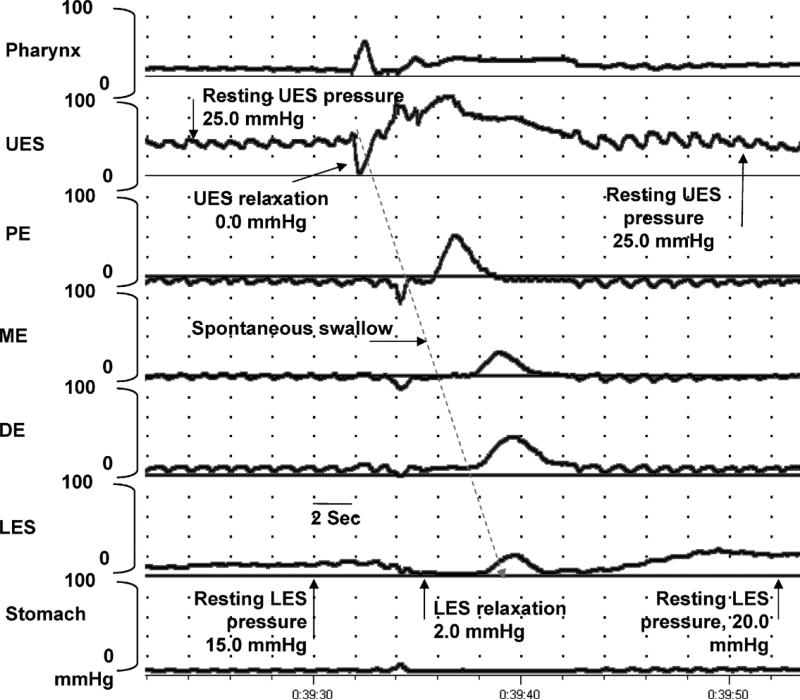
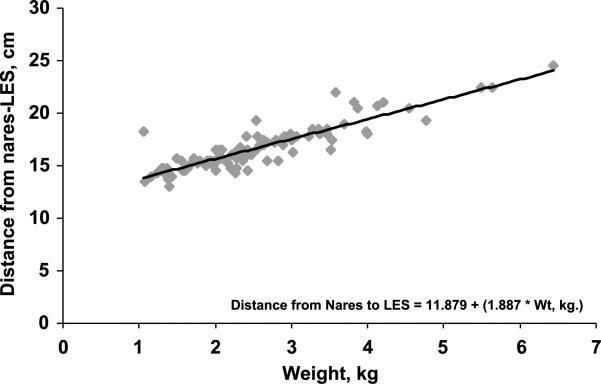
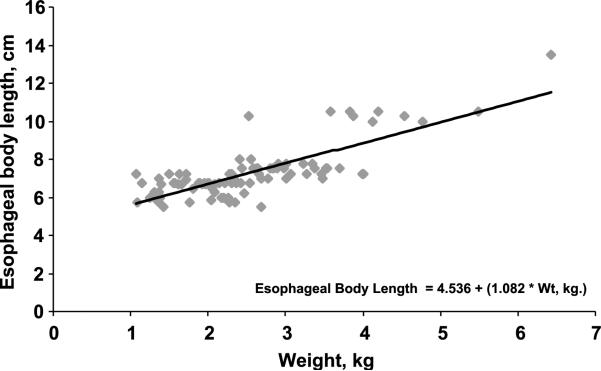
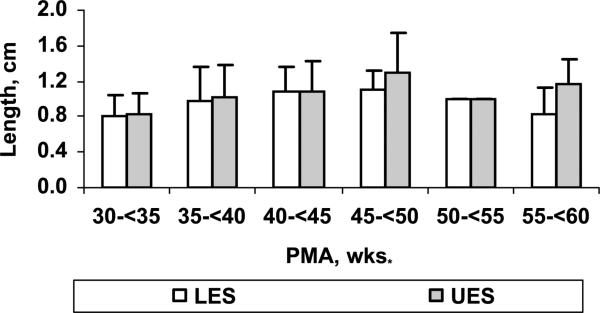
Design/methods: One hundred esophageal manometry studies were performed in 75 infants (30-60 weeks PMA) and the high-pressure zones of LES and UES identified. The distance from nares to LES and from nares to UES, esophageal body length, length of UES and LES derived from the manometry studies were correlated with somatic growth parameters. Growth rate of different esophageal segments was also determined in 26 subjects that underwent longitudinal studies. Analysis of variance and linear regression analysis were performed.
Results: Seventy-five neonates of 23.0-40.6 weeks gestational age (0.6-4.4 kg) were studied at 29.1-58.6 weeks PMA (1.0-6.4 kg). Significant correlation (P < 0.001) of PMA and physical growth parameters with the growth of nares-LES (R = 0.8), esophageal body length (R = 0.6) and nares-UES (R = 0.4) were noted. Nares-to-LES length increased at a rate of 0.25 cm/wk PMA during 33.0-36.0 weeks of age.
Conclusions: In vivo esophageal segmental lengths correlated strongly with somatic growth parameters and PMA in neonates. We speculate that this approach has many practical applications with the use of esophageal probes and catheters.
Figures
Similar articles
-
Neuromotor markers of esophageal motility in feeding intolerant infants with gastroschisis.J Pediatr Gastroenterol Nutr. 2008 Aug;47(2):158-64. doi: 10.1097/MPG.0b013e318162082f. J Pediatr Gastroenterol Nutr. 2008. PMID: 18664867
-
Gestational and postnatal modulation of esophageal sphincter reflexes in human premature neonates.Pediatr Res. 2015 Nov;78(5):540-6. doi: 10.1038/pr.2015.149. Epub 2015 Aug 13. Pediatr Res. 2015. PMID: 26270576 Free PMC article.
-
Balloon dilation of the esophago-gastric junction affects lower and upper esophageal sphincter function in achalasia.Neurogastroenterol Motil. 2014 Jan;26(1):69-76. doi: 10.1111/nmo.12228. Epub 2013 Sep 4. Neurogastroenterol Motil. 2014. PMID: 24004089
-
Development of pharyngo-esophageal physiology during swallowing in the preterm infant.Neurogastroenterol Motil. 2011 Oct;23(10):e401-8. doi: 10.1111/j.1365-2982.2011.01763.x. Epub 2011 Aug 9. Neurogastroenterol Motil. 2011. PMID: 21827583 Review.
-
The upper esophageal sphincter in the high-resolution manometry era.Langenbecks Arch Surg. 2021 Dec;406(8):2611-2619. doi: 10.1007/s00423-021-02319-1. Epub 2021 Aug 31. Langenbecks Arch Surg. 2021. PMID: 34462811 Review.
Cited by
-
Maturation of upstream and downstream esophageal reflexes in human premature neonates: the role of sleep and awake states.Am J Physiol Gastrointest Liver Physiol. 2013 Nov;305(9):G649-58. doi: 10.1152/ajpgi.00002.2013. Epub 2013 Sep 5. Am J Physiol Gastrointest Liver Physiol. 2013. PMID: 24008357 Free PMC article.
-
Differentiating esophageal sensitivity phenotypes using pH-impedance in intensive care unit infants referred for gastroesophageal reflux symptoms.Pediatr Res. 2021 Feb;89(3):636-644. doi: 10.1038/s41390-020-0930-6. Epub 2020 May 6. Pediatr Res. 2021. PMID: 32375162 Free PMC article.
-
Impact of feeding strategies on the frequency and clearance of acid and nonacid gastroesophageal reflux events in dysphagic neonates.JPEN J Parenter Enteral Nutr. 2012 Jul;36(4):449-55. doi: 10.1177/0148607111415980. Epub 2011 Oct 30. JPEN J Parenter Enteral Nutr. 2012. PMID: 22038208 Free PMC article.
-
The Role of Sleep in the Modulation of Gastroesophageal Reflux and Symptoms in NICU Neonates.Pediatr Neurol. 2015 Sep;53(3):226-32. doi: 10.1016/j.pediatrneurol.2015.05.012. Epub 2015 May 29. Pediatr Neurol. 2015. PMID: 26149107 Free PMC article.
-
Continuous versus bolus intermittent intragastric tube feeding for preterm and low birth weight infants with gastro-oesophageal reflux disease.Cochrane Database Syst Rev. 2021 Aug 6;8(8):CD009719. doi: 10.1002/14651858.CD009719.pub3. Cochrane Database Syst Rev. 2021. PMID: 34355390 Free PMC article.
References
-
- DiLorenzo C, Hillemeier C, Hyman P, et al. Manometry studies in children: minimum standards for procedures. Neurogastroenterol Motil. 2002;14:411–20. (Review) - PubMed
-
- Emmerson AJ, Chant T, May J, Vales P. Assessment of three methods of pH probe positioning in preterm infants. J Pediatr Gastroenterol Nutr. 2002;35:69–72. - PubMed
-
- American Gastroenterological Association Medical Position Statement: guidelines on the use of esophageal PH recording. Gastroenterology. 1996;110:1981. - PubMed
-
- Klauser AG, Schindlbeck NE, Müller-Lissner SA. Esophageal 24-hour pH monitoring: is prior manometry necessary for correct positioning of the electrode? Am J Gastroenterol. 1990;85:1463–7. - PubMed
-
- Pehl C, Boccali I, Hennig M, Schepp W. pH probe positioning for 24-hour pH-metry by manometry or pH step-up. Eur J Gastroenterol Hepatol. 2004;16:375–82. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
