

The potential impact of male circumcision on HIV in Sub-Saharan Africa
- PMID: 16822094
- PMCID: PMC1489185
- DOI: 10.1371/journal.pmed.0030262
The potential impact of male circumcision on HIV in Sub-Saharan Africa
Abstract
Background: A randomized controlled trial (RCT) has shown that male circumcision (MC) reduces sexual transmission of HIV from women to men by 60% (32%-76%; 95% CI) offering an intervention of proven efficacy for reducing the sexual spread of HIV. We explore the implications of this finding for the promotion of MC as a public health intervention to control HIV in sub-Saharan Africa.
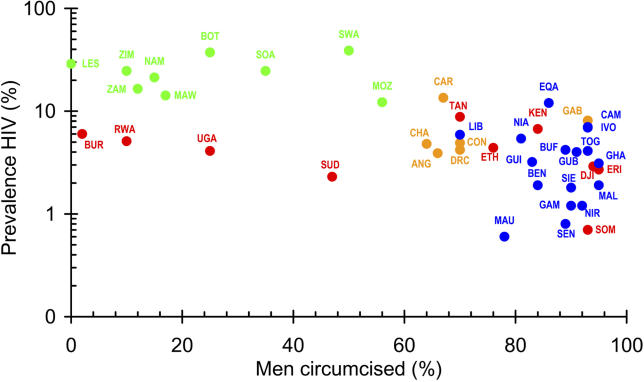
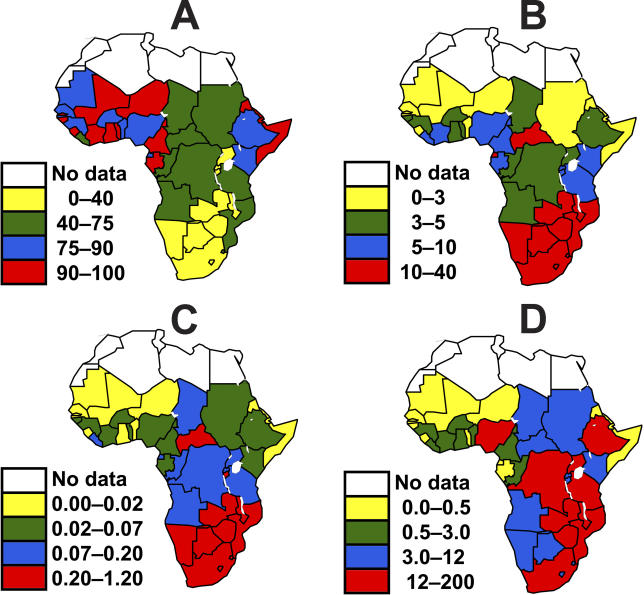
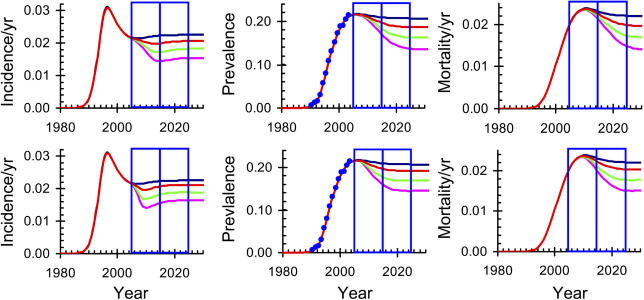
Methods and findings: Using dynamical simulation models we consider the impact of MC on the relative prevalence of HIV in men and women and in circumcised and uncircumcised men. Using country level data on HIV prevalence and MC, we estimate the impact of increasing MC coverage on HIV incidence, HIV prevalence, and HIV-related deaths over the next ten, twenty, and thirty years in sub-Saharan Africa. Assuming that full coverage of MC is achieved over the next ten years, we consider three scenarios in which the reduction in transmission is given by the best estimate and the upper and lower 95% confidence limits of the reduction in transmission observed in the RCT. MC could avert 2.0 (1.1-3.8) million new HIV infections and 0.3 (0.1-0.5) million deaths over the next ten years in sub-Saharan Africa. In the ten years after that, it could avert a further 3.7 (1.9-7.5) million new HIV infections and 2.7 (1.5-5.3) million deaths, with about one quarter of all the incident cases prevented and the deaths averted occurring in South Africa. We show that a) MC will increase the proportion of infected people who are women from about 52% to 58%; b) where there is homogenous mixing but not all men are circumcised, the prevalence of infection in circumcised men is likely to be about 80% of that in uncircumcised men; c) MC is equivalent to an intervention, such as a vaccine or increased condom use, that reduces transmission in both directions by 37%.
Conclusions: This analysis is based on the result of just one RCT, but if the results of that trial are confirmed we suggest that MC could substantially reduce the burden of HIV in Africa, especially in southern Africa where the prevalence of MC is low and the prevalence of HIV is high. While the protective benefit to HIV-negative men will be immediate, the full impact of MC on HIV-related illness and death will only be apparent in ten to twenty years.
Conflict of interest statement
Figures
References
-
- WHO, UNAIDS. Progress on access to anti-retroviral therapy: An update on “3 by 5.” Geneva: World Health Organization. 34 p. 2005
-
- USAID. The President's emergency plan for AIDS relief: US five-year Global HIV/AIDS strategy. 2004 Available: http://www.usaid.gov/our_work/global_health/aids/pepfar.html. Accessed 25 May 2006 .
-
- Wilson PA, Binagwaho A, Ruxin J. Combating AIDS in the developing world. London: Earthscan; 2005. 276 pp.
-
- Carael M, Holmes K, editors. The multicentre study of factors determining the different prevalences of HIV in sub-Saharan Africa. AIDS. 2001;15:S1–S132.
