

The risk of death associated with delayed coronary artery bypass surgery
- PMID: 16822309
- PMCID: PMC1574305
- DOI: 10.1186/1472-6963-6-85
The risk of death associated with delayed coronary artery bypass surgery
Abstract
Background: The detrimental effect of delaying surgical revascularization has been estimated in randomized trials and observational studies. It has been argued that the Kaplan-Meier method used in quantifying the hazard of delayed treatment is not appropriate for summarizing the probability of competing outcomes. Therefore, we sought to improve the estimates of the risk of death associated with delayed surgical treatment of coronary artery disease.
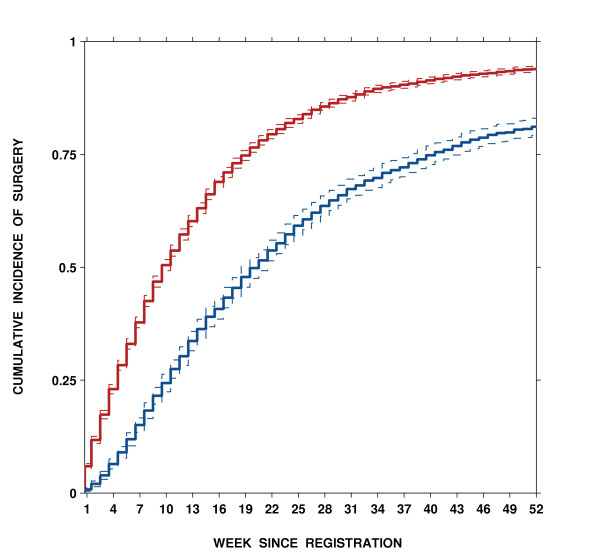
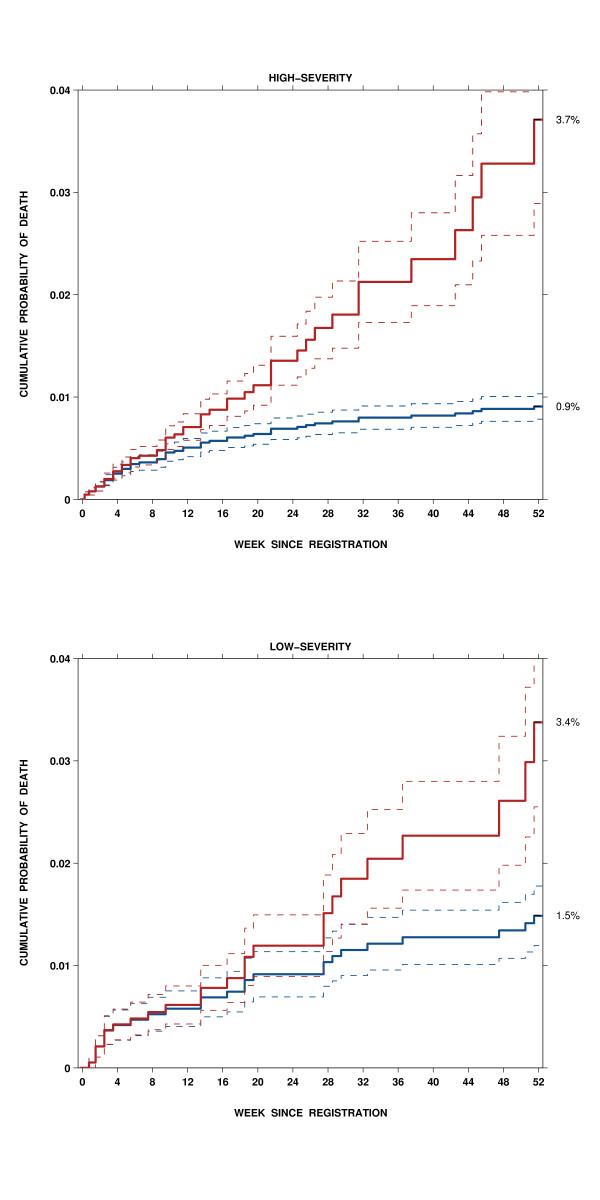
Methods: Population-based prospective study of 8,325 patients registered to undergo first time isolated coronary artery bypass grafting (CABG) in any of the four tertiary hospitals that provide cardiac care to adult residents of British Columbia, Canada. The cumulative incidence of pre-operative death, the cumulative incidence of surgery, and the probability that a patient, who may die or undergo surgery, dies if not operated by certain times over the 52-week period after the decision for CABG were estimated. The risks were quantified separately in two groups: high-severity at presentation were patients with either persistent unstable angina or stable angina and extensive coronary artery disease, and low-severity at presentation were stable symptomatic patients with limited disease.
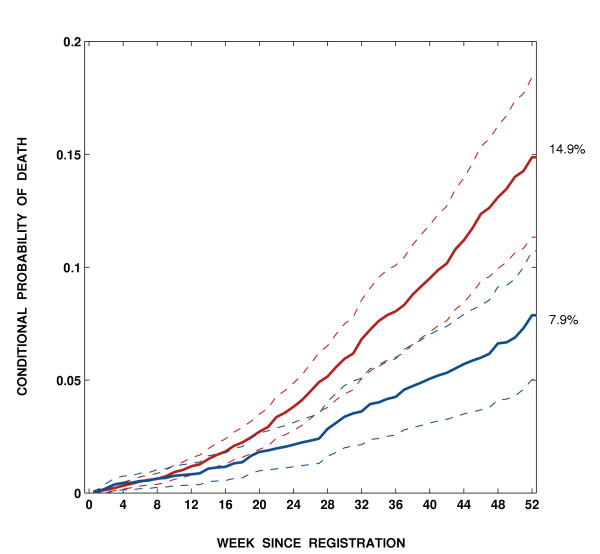
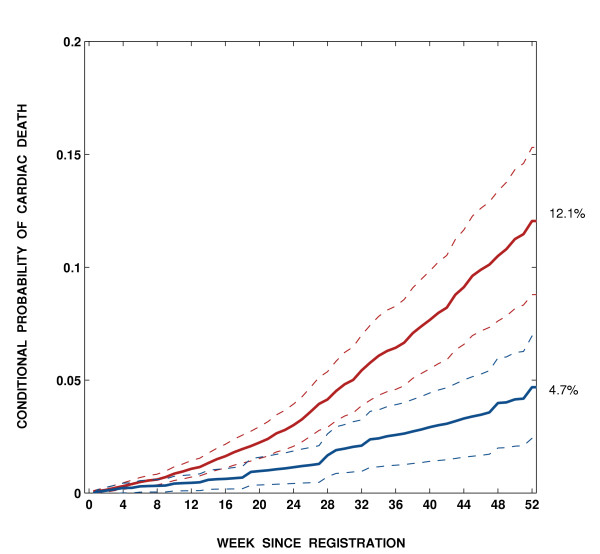
Results: The median waiting time for surgery was 10 weeks (interquartile range [IQR] 15 weeks) in the high-severity group and 21 weeks (IQR 30 weeks) in the low-severity group. One percent of patients died before surgery: 54 in the high-severity and 26 in the low-severity group. For 58 (72.5%) patients, death was related to CVD (acute coronary syndrome, 33; chronic CVD, 16; other CVD, 4; and sudden deaths, 5). The overall death rate from all causes was 0.61 (95% CI 0.48-0.74) per 1,000 patient-weeks, varying from 0.62 (95% CI 0.45-0.78) in the high-severity group to 0.59 (95% CI 0.37-0.82) in the low-severity group. After adjustment for age, sex, and comorbidity, the all-cause death rate in the low-severity group was similar to the high-severity group (OR = 1.02, 95% CI 0.64-1.62). The conditional probability of death was greater in the high-severity group than in the low-severity group both for all-cause mortality (p = 0.002) and cardiovascular deaths (p <0.001).
Conclusion: The probability of death conditional on not having undergone a required CABG increases with time spent on wait lists.
Figures
Similar articles
-
Do longer delays for coronary artery bypass surgery contribute to preoperative mortality in less urgent patients?Med Care. 2006 Jul;44(7):680-6. doi: 10.1097/01.mlr.0000220257.81482.67. Med Care. 2006. PMID: 16799363
-
Cumulative incidence for wait-list death in relation to length of queue for coronary-artery bypass grafting: a cohort study.J Cardiothorac Surg. 2006 Aug 24;1:21. doi: 10.1186/1749-8090-1-21. J Cardiothorac Surg. 2006. PMID: 16930475 Free PMC article.
-
Delay in admission for elective coronary-artery bypass grafting is associated with increased in-hospital mortality.BMC Health Serv Res. 2008 Sep 19;8:185. doi: 10.1186/1472-6963-8-185. BMC Health Serv Res. 2008. PMID: 18803823 Free PMC article.
-
Percutaneous coronary intervention or coronary artery bypass surgery for cardiogenic shock and multivessel coronary artery disease?Am Heart J. 2010 Jan;159(1):141-7. doi: 10.1016/j.ahj.2009.10.035. Am Heart J. 2010. PMID: 20102880 Review.
-
Long-term outcome of a routine versus selective invasive strategy in patients with non-ST-segment elevation acute coronary syndrome a meta-analysis of individual patient data.J Am Coll Cardiol. 2010 Jun 1;55(22):2435-45. doi: 10.1016/j.jacc.2010.03.007. Epub 2010 Mar 30. J Am Coll Cardiol. 2010. PMID: 20359842 Review.
Cited by
-
Overestimation of the probability of death on peritoneal dialysis by the Kaplan-Meier method: advantages of a competing risks approach.BMC Nephrol. 2012 May 30;13:31. doi: 10.1186/1471-2369-13-31. BMC Nephrol. 2012. PMID: 22646159 Free PMC article.
-
English NHS waiting times: what next?J R Soc Med. 2009 Jul;102(7):260-4. doi: 10.1258/jrsm.2009.090044. J R Soc Med. 2009. PMID: 19605856 Free PMC article. No abstract available.
-
Effects of Wait Times on Treatment Adherence and Clinical Outcomes in Patients With Severe Sleep-Disordered Breathing: A Secondary Analysis of a Noninferiority Randomized Clinical Trial.JAMA Netw Open. 2020 Apr 1;3(4):e203088. doi: 10.1001/jamanetworkopen.2020.3088. JAMA Netw Open. 2020. PMID: 32310283 Free PMC article. Clinical Trial.
-
The effect of coronary revascularization treatment timing on mortality in patients with stable ischemic heart disease in British Columbia.PLoS One. 2024 Oct 24;19(10):e0303222. doi: 10.1371/journal.pone.0303222. eCollection 2024. PLoS One. 2024. PMID: 39446787 Free PMC article.
-
Multimodal prehabilitation as strategy for reduction of postoperative complications after cardiac surgery: a randomised controlled trial protocol.BMJ Open. 2020 Dec 22;10(12):e039885. doi: 10.1136/bmjopen-2020-039885. BMJ Open. 2020. PMID: 33371022 Free PMC article. Clinical Trial.
References
-
- Yusuf S, Zucker D, Peduzzi P, Fisher LD, Takaro T, Kennedy JW, Davis K, Killip T, Passamani E, Norris R. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet. 1994;344:563–570. doi: 10.1016/S0140-6736(94)91963-1. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
